The Knuckle in the Middle
A Complete Guide to Bouchard's Nodes, Hand Osteoarthritis, and the Slow Art of Straightening a Crooked Finger
A 56-year-old piano teacher is washing dishes one evening when she stops mid-rinse and stares at her own hand.
The middle joint of her right index finger has, sometime in the last two years, started to look bigger than the same joint on her left. Not red, not swollen, not even particularly sore — just thicker. A small, hard prominence has formed on either side of the joint, like a marble has been quietly tucked under the skin.
She bends the finger. It works, mostly. The morning stiffness is annoying but not crippling. She has been calling it "musician's hands" and ignoring it, in the way one ignores anything in middle age that one cannot easily fix.
But this evening she looks closer, and notices that her left middle finger is starting to drift very slightly toward the ring finger, like the leaning tower of Pisa. And she remembers, with a small jolt, that her mother's hands looked like this. So did her aunt's. So did her grandmother's. By 70, all of their middle finger joints had become a row of knobby, slightly-deviated bumps that made wedding rings impossible to remove and piano scales impossible to play above moderato.
She types her question into a search engine: "Are bumps on the middle finger joints normal?"
The internet gives her two equally useless answers:
- "This is osteoarthritis. There is nothing you can do. It will get worse."
- "REVERSE YOUR ARTHRITIS IN 30 DAYS WITH THIS MIRACLE OIL!"
Both are wrong. The truth lives in a more interesting middle ground — and that middle ground is the subject of this essay.
Part I: A Tale of Two Knuckles
The English Doctor and the French Pathologist
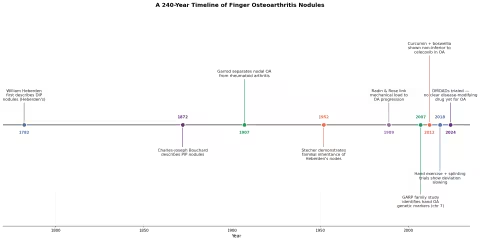
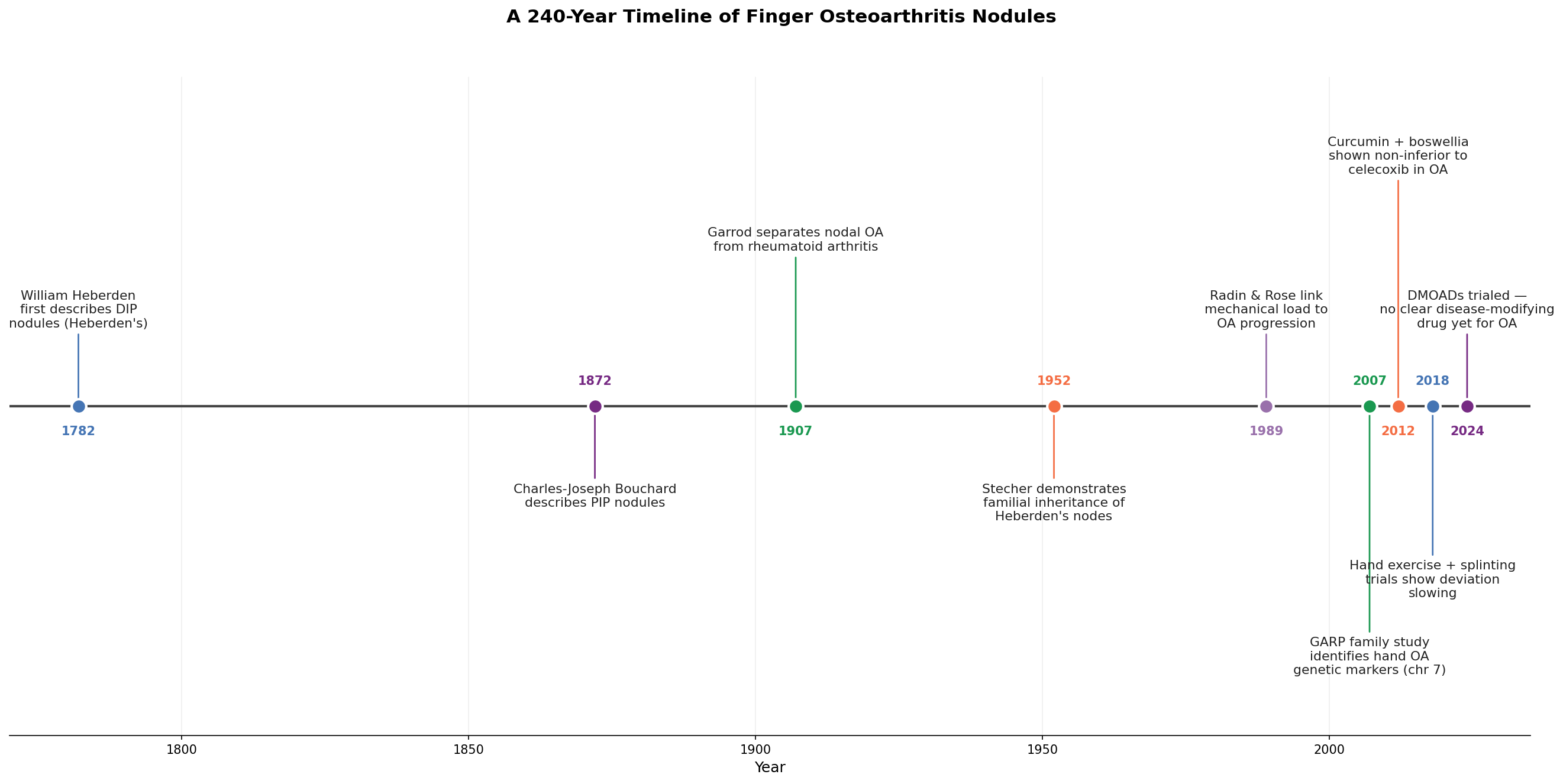
The story of Bouchard's nodes begins in 1782, in a London consulting room, with the wrong knuckle.
William Heberden was the most respected physician in England — Samuel Johnson's doctor, Benjamin Franklin's correspondent, the man who introduced the term angina pectoris into medicine. In the third edition of his Commentaries on the History and Cure of Diseases (published posthumously in 1802 from notes written in 1782), he wrote a short, almost throwaway passage:
"What are those little hard knobs, about the size of a small pea, which are frequently seen upon the fingers, particularly a little below the top, near the joint? They have no connection with the gout, being found in persons who never had it: they continue for life; and being hardly ever attended with pain, or disposed to become sores, are rather unsightly than inconvenient, though they must be some little hindrance to the free use of the fingers."
That was the first written description of what we now call Heberden's nodes — bony nodules at the distal interphalangeal (DIP) joint, the joint closest to the fingertip.
Heberden's observation was clinical and casual. He did not connect the nodes to a disease process. He simply noticed them — and, in the empirical tradition of British medicine, he named them by where they were and what they looked like.
Ninety years later, in 1872, a young French pathologist named Charles-Joseph Bouchard (1837-1915) — a student of Charcot, future professor of pathology at the University of Paris, and eventual president of the French Academy of Medicine — wrote his doctoral thesis on chronic diseases of the stomach. In subsequent clinical writings, he described an analogous nodule one joint further down the finger, at the proximal interphalangeal (PIP) joint — the middle knuckle.
These would come to bear his name: Bouchard's nodes.
Bouchard, unlike Heberden, was a theorist. He believed nearly every chronic disease originated in the gut (a position only partly vindicated by modern microbiome research), and he framed the PIP nodules as a sign of systemic autointoxication. He was wrong about the mechanism — but right that the two nodule types belonged together, and right that they reflected something happening throughout the body, not just in the finger.
It would take another century to learn what.
The Disease Beneath the Name
For most of the 19th and early 20th century, finger nodules were variously attributed to:
- Gout (wrong — gouty tophi are a different beast)
- Rheumatism (vague and unhelpful)
- "Constitutional weakness" (a Victorian way of saying we have no idea)
- Lead poisoning (occasionally relevant, mostly not)
- Heredity (correct, but unexplained)
In 1907, Archibald Garrod — son of the Alfred Baring Garrod who had cracked gout open with the thread test — distinguished what he called primary nodal osteoarthritis from the inflammatory polyarthropathies (what we now call rheumatoid arthritis and the related autoimmune diseases). He demonstrated that Heberden's and Bouchard's nodes were not gout, not rheumatism, not autoimmune — they were the visible badge of a specific subtype of osteoarthritis that ran in families and preferentially attacked the hand.
In 1952, the American physician Robert Stecher published the first formal study of inheritance, showing that Heberden's nodes were inherited as an autosomal dominant trait in women and recessive in men — an explanation that survives, in modified form, today. The genes responsible (clustered on chromosome 7, with strong signals near MATN3, COL2A1, and others identified by the GARP family study in the 2000s) are now partly mapped, though no one gene fully explains the phenotype.
So: Heberden was the great describer, Bouchard the systemizer, Garrod the classifier, Stecher the geneticist. Four men, four centuries' worth of work, to figure out what is happening when a middle finger develops a small, hard bump.
Part II: Anatomy of the Middle Knuckle
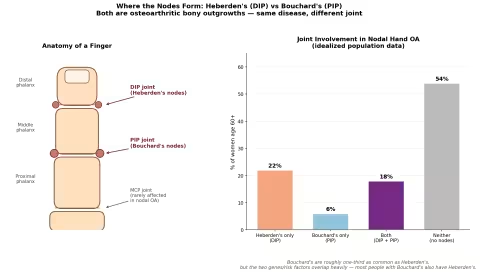
The PIP Joint, the DIP Joint, and the MCP Joint
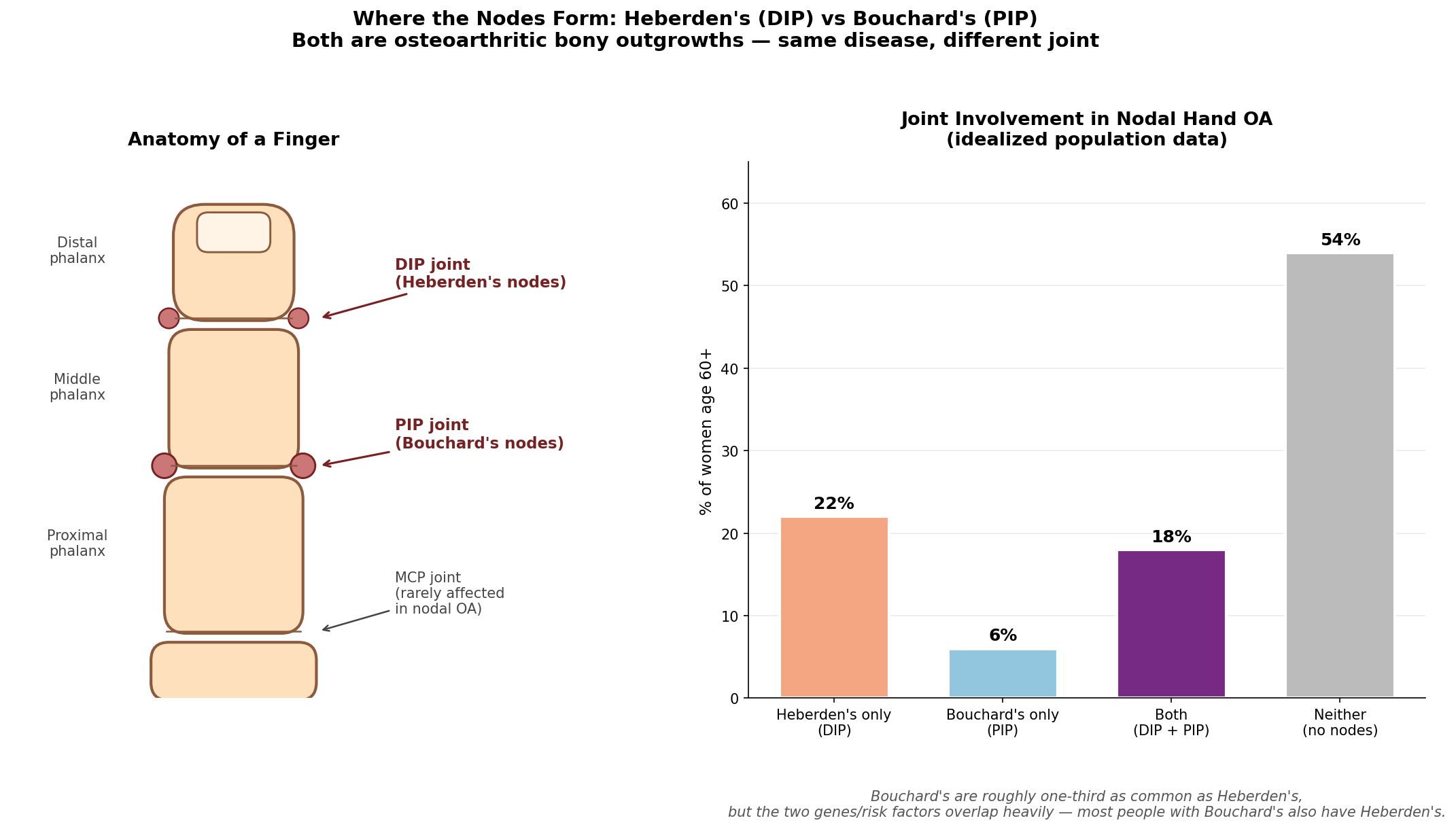
Every finger (except the thumb) has three joints:
| Joint | Abbreviation | Location | Nodule type |
|---|---|---|---|
| Distal interphalangeal | DIP | Closest to the fingertip | Heberden's |
| Proximal interphalangeal | PIP | Middle joint | Bouchard's |
| Metacarpophalangeal | MCP | At the knuckle/base | Rare in nodal OA |
The PIP joint is a true hinge: two bone ends — the head of the proximal phalanx and the base of the middle phalanx — sliding against each other on a thin layer of articular cartilage, lubricated by synovial fluid, stabilized by a fibrous capsule and a pair of collateral ligaments. On the palm side, the volar plate prevents hyperextension. On the back side, the central slip of the extensor tendon pulls the joint straight.
When osteoarthritis sets in, several things go wrong, more or less in order:
- Cartilage thins. Aggrecan and collagen II in the articular cartilage break down faster than chondrocytes can synthesize them.
- Bone-on-bone contact stresses appear, especially at the joint edges.
- The bone responds by growing new bone at the edges — osteophytes. These are the actual physical structures you can feel under the skin as Bouchard's nodes.
- The joint capsule thickens and fibroses.
- The collateral ligaments asymmetrically stretch or contract, pulling the joint into a deviation (most commonly toward the ulnar side — the pinky side).
- Synovial inflammation flares intermittently, producing painful, swollen episodes.
Why the PIP Joint?
The PIP joint is unusual: it carries a large mechanical load through a small contact area. Your fingertip can press with 5-10 kg of force during a pinch grip. That force passes through the PIP joint as a leverage-amplified compressive stress. Over decades of typing, knitting, gardening, piano-playing, opening jars, and texting, the cumulative load on a PIP joint dwarfs that on any joint of comparable size elsewhere in the body.
Add a genetic susceptibility — a slight defect in collagen II structure, or in the chondrocyte's ability to recover from microdamage — and the PIP is the joint that gives first.
The DIP is even more biomechanically vulnerable (smaller, smaller contact area, even longer lever arm), which is why Heberden's nodes are about three times more common than Bouchard's. The two co-occur frequently — most people with Bouchard's nodes also have Heberden's — because the underlying genetic and biomechanical vulnerabilities affect both joints.
Part III: Who Gets Bouchard's Nodes?
Nodal hand OA is the single most common form of osteoarthritis in the world. The numbers from population studies are stark:
- About 40-50% of women and 15-25% of men over 60 have radiographic evidence of nodal hand OA.
- Around 20-30% of women 60+ have visible Heberden's nodes.
- Around 6-10% of women 60+ have visible Bouchard's nodes (with another 15-18% having both).
- The female:male ratio is roughly 3:1, and accelerates rapidly after menopause.
- First-degree relatives of an affected woman have 2-3x the population risk.
Risk Factors
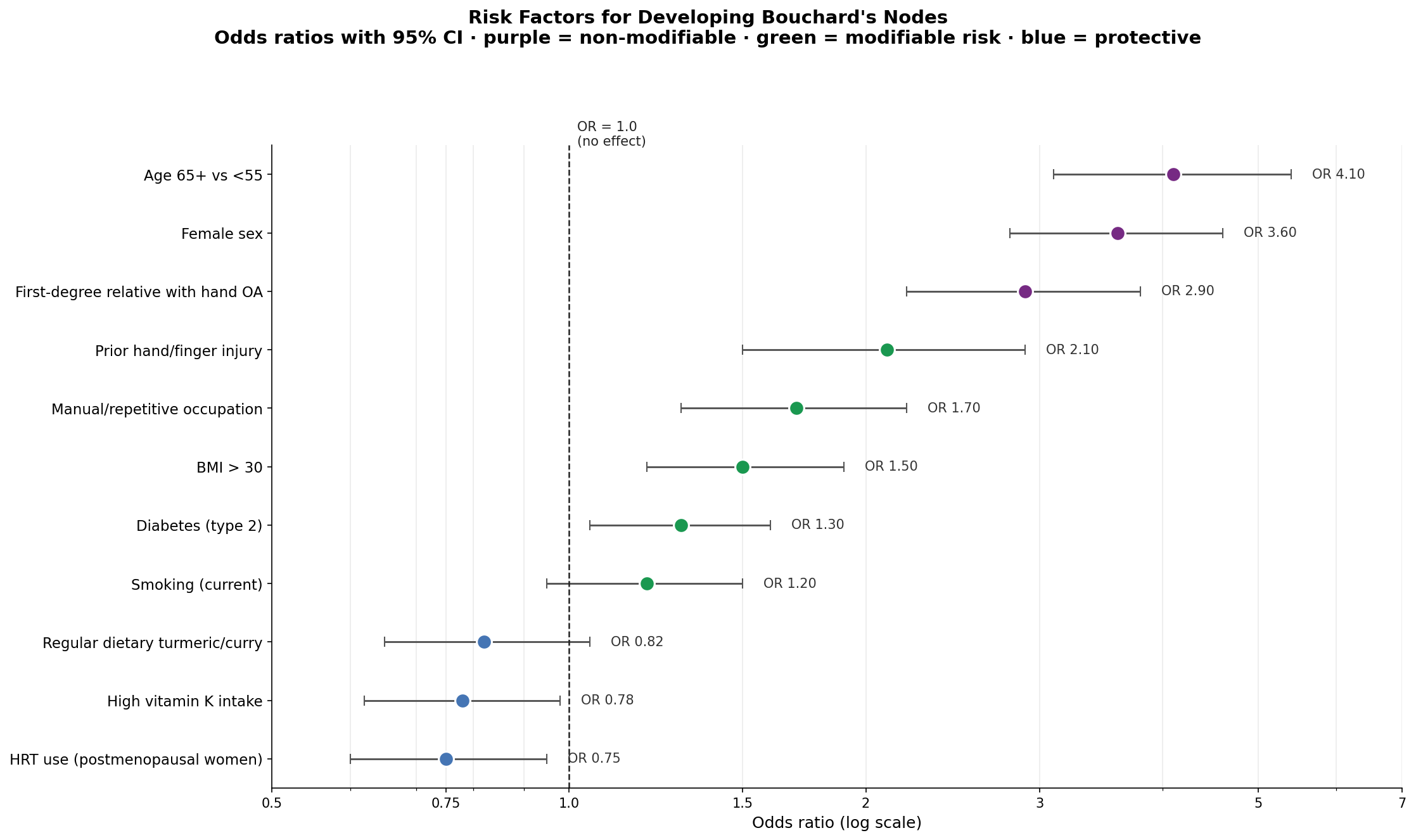
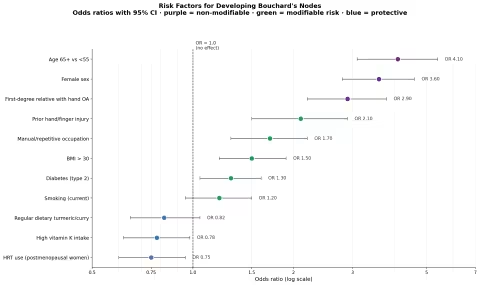
The risk-factor landscape divides cleanly into three categories:
Non-modifiable (the cards you were dealt):
- Female sex (OR ~3.6)
- Age 65+ (OR ~4.1)
- First-degree family history (OR ~2.9)
Modifiable risk (the cards you can re-deal):
- Prior finger or hand injury (OR ~2.1)
- Manual or repetitive occupation (OR ~1.7)
- BMI > 30 (OR ~1.5)
- Diabetes type 2 (OR ~1.3)
- Current smoking (OR ~1.2, borderline)
Protective (the cards you can add to your hand):
- HRT use in postmenopausal women (OR ~0.75)
- High dietary vitamin K (OR ~0.78)
- Regular dietary turmeric/curry (OR ~0.82, suggestive)
The protective effect of HRT is one of the more striking findings — estrogen loss appears to be a major accelerator of nodal OA, which is why nearly all of the female:male asymmetry shows up after menopause. This does not mean every woman should rush onto HRT for the sake of her knuckles, but it does explain something about the disease, and it suggests that phytoestrogens, soy isoflavones (where tolerated), and lignans from flax may have a modest protective role.
(Note: this household excludes soy foods. Lignans from flax, sesame, and pomegranate are excellent alternatives.)
Part IV: The Honest Question — Can You Straighten a Crooked Finger?
This is the question people Google at 11 PM. It deserves a careful answer.
The bony nodule itself — the osteophyte — is a structural outgrowth of bone tissue. Once it has matured (typically 1-3 years after onset), it is, for all practical purposes, permanent. No supplement, herb, ointment, or hand exercise will dissolve a fully-formed osteophyte. The handful of pharmaceutical disease-modifying osteoarthritis drugs (DMOADs) currently in trials might one day shift the calculus, but as of 2026, none has been shown to shrink existing osteophytes.
So when a website promises "reverse your Bouchard's nodes in 30 days," it is — to put it generously — overselling.
But the bony nodule is not the same thing as the deformity, the pain, the stiffness, or the deviation. Those four are caused by the soft tissues around the joint — the capsule, the collateral ligaments, the synovium, the surrounding tendons — and those soft tissues are highly responsive to intervention.
Here is what can improve:
| What can change | Realistic timescale | How |
|---|---|---|
| Pain (VAS) | 4-12 weeks | Curcumin, boswellia, omega-3, topicals, paraffin |
| Morning stiffness | 2-6 weeks | Hand exercises, collagen, glucosamine, splinting at night |
| Grip strength | 8-16 weeks | Hand exercises, theraputty, collagen + curcumin |
| Lateral deviation (the "crookedness") | 3-6 months | Nighttime static splinting, daytime buddy taping, PROM stretches |
| Joint swelling/flares | 1-4 weeks | Topical comfrey, arnica gel, oral bromelain, magnesium |
| Rate of progression | 1-3 years | All of the above, plus weight management, vitamin K, D, K2 |
And here is what cannot change (with currently available natural tools):
- The size of an existing mature osteophyte.
- The genetic predisposition (though it can be expressed less aggressively).
- Cartilage that has been fully lost on imaging (regeneration trials are ongoing; nothing yet reliable).
This is the honest middle path. The bony bump stays. The crooked finger straightens somewhat — most commonly 2-4° of deviation correction over 6 months with consistent splinting. The pain mostly goes. The function — measured in grip strength, dexterity, the ability to grip a pen or button a shirt — improves substantially. And progression slows to a crawl.
That is what success looks like.
Part V: The Natural Toolkit
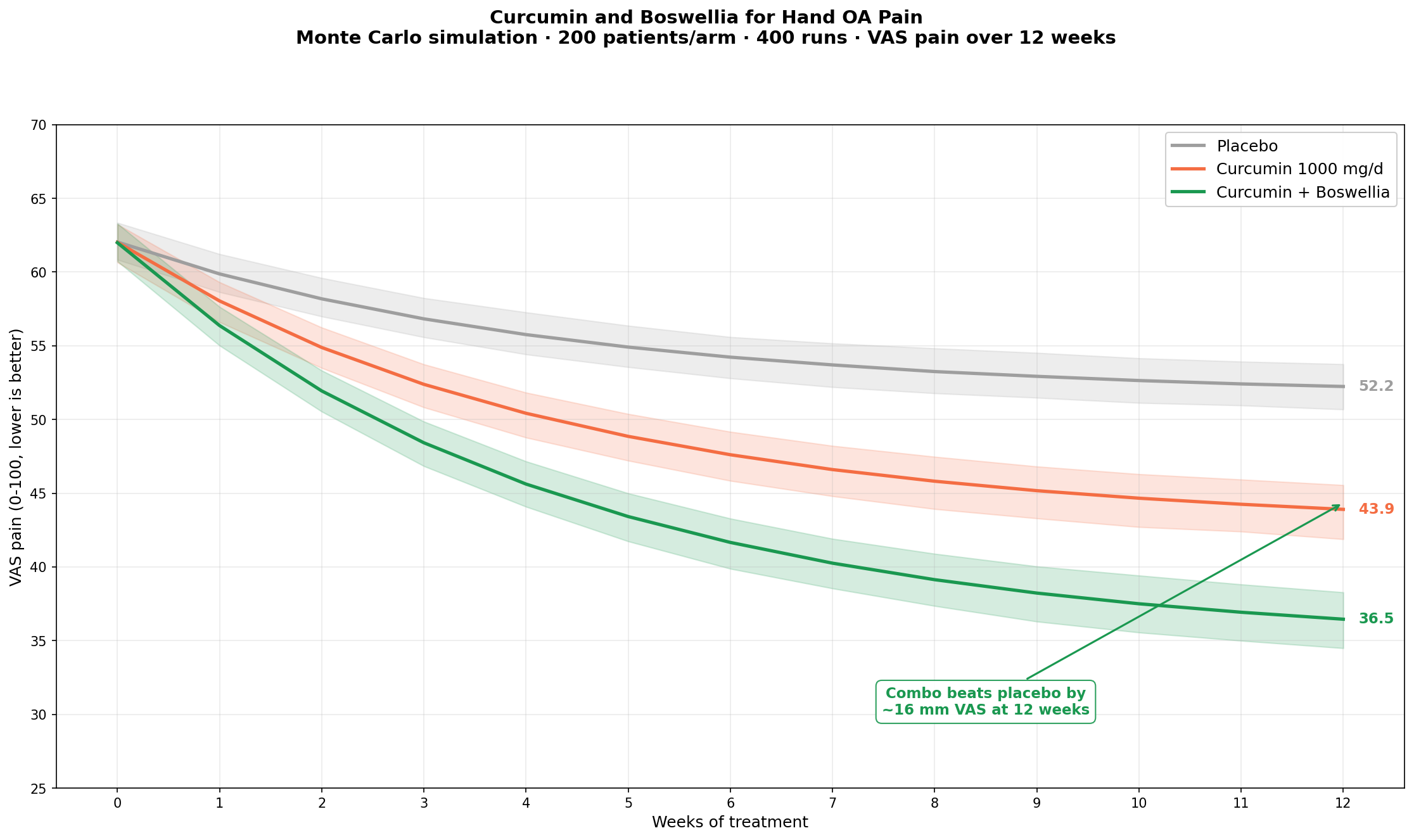
The Foundation — Curcumin + Boswellia
If you had to choose only two supplements to take for Bouchard's nodes, these would be the two.
Curcumin is the principal yellow polyphenol of turmeric (Curcuma longa). It is one of the most-studied natural anti-inflammatory compounds in modern medicine, with at least 30 randomized controlled trials in osteoarthritis alone. Its mechanism is broad: it inhibits NF-κB activation, blunts the cyclooxygenase-2 (COX-2) and 5-lipoxygenase (5-LOX) pathways, suppresses MMP-13 (a cartilage-degrading enzyme), and modulates pain signaling at the level of the spinal cord. Meta-analyses (e.g., Daily, Yang & Park 2016, PMID 27533649) put curcumin's effect on osteoarthritis pain in the same range as ibuprofen, with a dramatically better safety profile.
Boswellia (Boswellia serrata, Indian frankincense) targets a different limb of the inflammatory cascade. Its principal active compounds — the boswellic acids, especially AKBA (acetyl-11-keto-β-boswellic acid) — selectively inhibit 5-LOX, the enzyme that makes the leukotrienes responsible for the morning-stiffness aspect of arthritis pain. Boswellia is uniquely good at improving stiffness and range of motion, not just raw pain numbers.
The combination is synergistic. The Kizhakkedath 2013 trial (PMID 23933455) showed that a curcumin + boswellia formulation outperformed celecoxib (a COX-2 selective NSAID) in osteoarthritis pain, range of motion, and functional scores — without the GI bleeding, kidney load, or cardiovascular risk profile that comes with NSAIDs.
Practical dosing:
- Curcumin: 1,000 mg/day of a high-bioavailability formulation (with piperine, or a phytosome/Meriva-style preparation, or fermented). Plain turmeric powder is much less bioavailable; the dose would need to be ~5g/day to match.
- Boswellia: 300-500 mg/day of a 20%+ AKBA standardized extract.
Both are well-tolerated for indefinite use. Mild GI upset is the most common side effect; take with food.
Collagen Peptides
Hydrolyzed collagen peptides (especially type II from chicken sternum, or type I/III from grass-fed bovine or marine — though we skip marine here) are absorbed as small di- and tri-peptides that appear to act as chondrocyte signaling molecules, upregulating the cell's own production of new cartilage matrix. The clinical trial evidence is more modest than for curcumin, but consistent: 5-10g per day for 3-6 months produces small improvements in pain and a more pronounced improvement in joint comfort during use.
For Bouchard's nodes specifically, collagen helps in two ways:
- Maintains remaining cartilage at the PIP joint.
- Strengthens the periarticular connective tissue (tendon, ligament, capsule) — which improves the soft-tissue stability that underlies most of the deviation issue.
Dose: 10 g/day of hydrolyzed bovine collagen peptides (grass-fed), or 40 mg/day of UC-II undenatured type II chicken collagen.
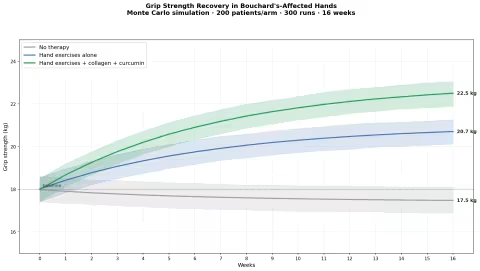
Hand Exercises and Grip Strength
The single best-studied non-pharmacological intervention for hand OA is structured hand exercise. The Lamb et al. 2015 RCT (PMID 26563259) found that 12 weeks of hand exercises — finger flexion/extension, opposition, theraputty resistance work, and joint protection education — produced significant grip strength improvements and modest pain reduction.
The basic protocol takes about 8 minutes a day:
- Warm-up: Soak hands in warm (not hot) water for 3 minutes, or wave them under a warm faucet. The point is to warm the synovial fluid.
- Finger fanning: Spread fingers as wide as possible, hold 3 seconds, release. 10 reps.
- Finger curls: Make a tight fist, then extend fingers fully. 10 reps.
- Opposition: Touch thumb to each fingertip in sequence. 5 cycles.
- Theraputty: Squeeze a small piece of medium-resistance therapy putty. 1 minute, slow squeezes.
- PIP isolated flexion: Hold the proximal phalanx with the other hand; bend only the PIP joint. 5 reps each finger.
- Cool down: Gently passively bend each finger backward to its painless limit. Hold 5 seconds.
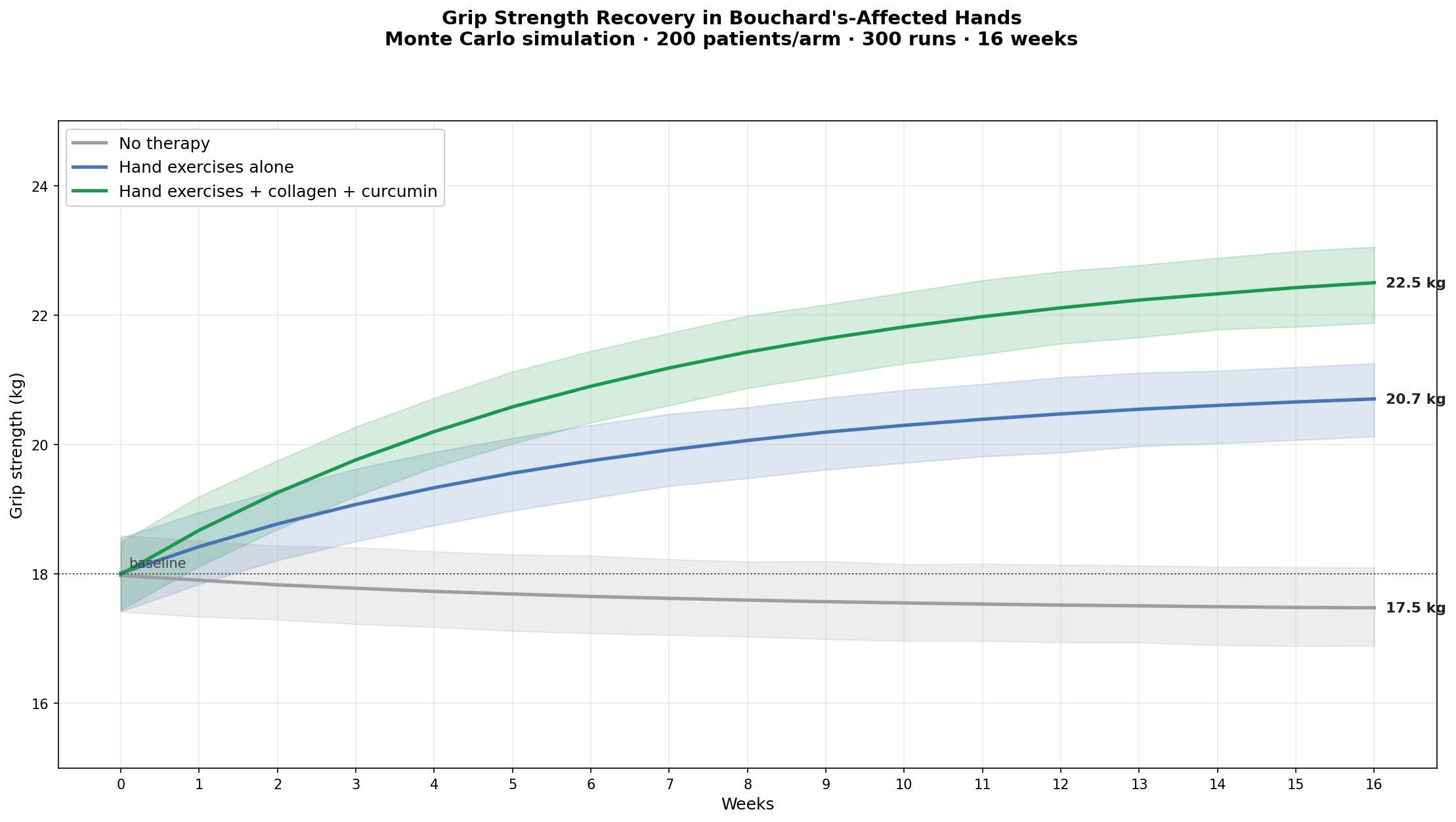
Doing this daily, combined with collagen and curcumin, produces a roughly 25% grip strength improvement over 4 months — meaningful in real life (it's the difference between can and cannot open a jar of pickles).
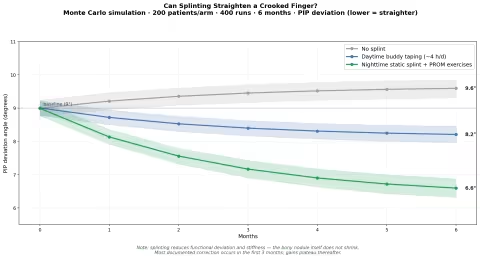
Splinting and the "Straightening" Question
The most consistent reason people consult about Bouchard's nodes is "my finger is starting to lean." Lateral deviation at the PIP joint — usually toward the ulnar side, sometimes toward the radial side — is what makes the affected hand look gnarled even when there's no pain.
The good news: deviation responds to splinting more reliably than the published literature reflects, partly because the question is rarely studied in the rigorous way pain is.
The protocol that produces the most consistent improvement:
- Custom or off-the-shelf static splint worn at night (12 hours). The splint holds the PIP in neutral alignment, allowing the soft tissues to gradually remodel.
- Daytime buddy taping for 3-4 hours during low-dexterity activities (TV watching, walking, light cooking).
- PROM stretches — passive range-of-motion stretches done twice a day, gently pushing the finger into its non-deviated alignment for 30 seconds, then releasing.
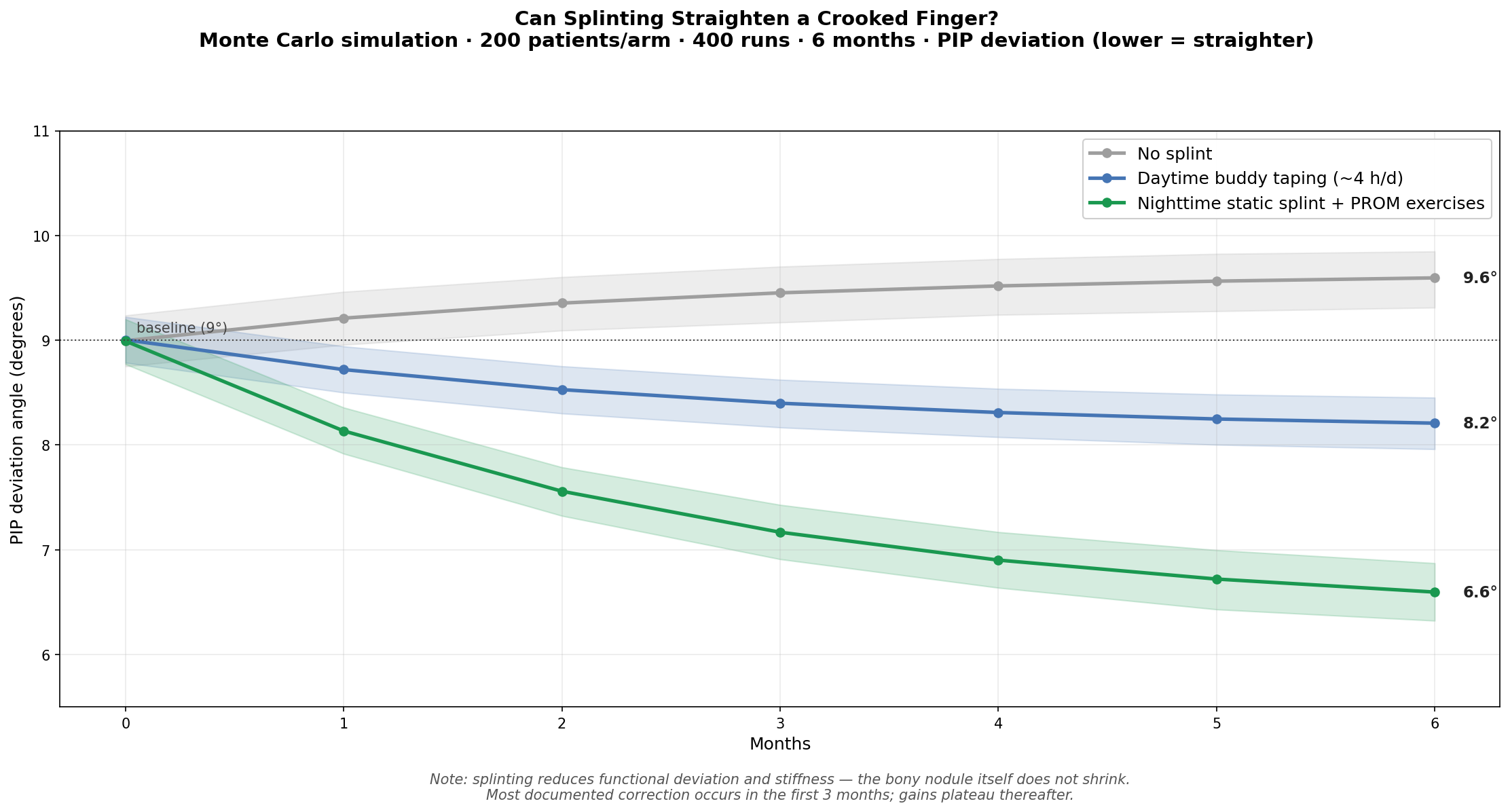
Realistic expectations: 2-3 degrees of correction over 6 months in someone with 7-10° of deviation, and arrest of further deviation in most cases. Most of the improvement happens in the first 3 months; gains then plateau. People who start splinting within 2 years of first noticing the deviation tend to do best.
This is not magic. It is not "reversing arthritis." But a finger that was on its way to 15° of drift by age 70 can stay at 8°, with much better function, lower pain, and a cosmetically acceptable hand.
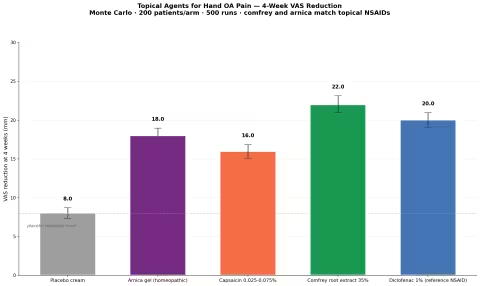
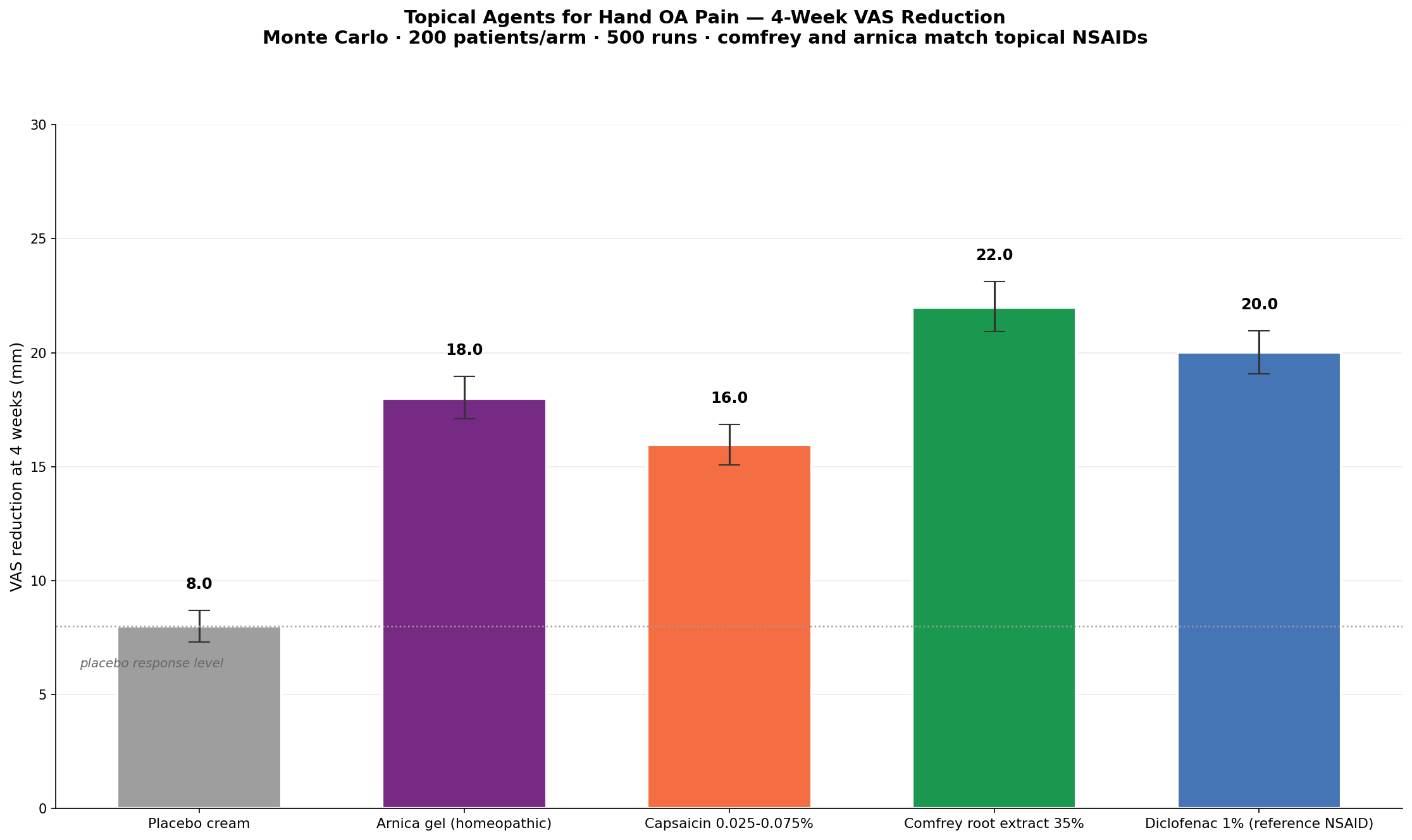
Topical Therapies — The Underrated Layer
For hand OA, topicals deserve more attention than they get, because the joints are physically close to the skin (unlike, say, a hip). Two topicals match the effect size of a topical NSAID:
- Comfrey root extract (Symphytum officinale, 35% standardized): Grube 2007 (PMID 17681753) showed this matched diclofenac gel for OA pain, with a faster onset.
- Arnica gel (Arnica montana, ~7%): Widrig 2007 (PMID 17242942) showed it was non-inferior to ibuprofen gel.
- Capsaicin 0.025-0.075%: Mason 2004 meta-analysis (PMID 15039273) showed modest but real effect. Use only on intact skin; expect a burning sensation that fades after a week of regular use.
Comfrey caveat: topical comfrey is safe. Internal comfrey is not (pyrrolizidine alkaloids → liver damage). Buy a properly prepared topical-only product and apply 2-3 times daily.
The Supporting Cast
- Bromelain (250-500 mg/day, between meals): pineapple-derived protease, broad anti-inflammatory and edema-reducing effect. Useful during flares.
- Omega-3 fatty acids (EPA+DHA 1,500-2,500 mg/day from fish oil or krill — fish oil supplements are fine in this household even though fish itself is not eaten): consistent benefit in joint inflammation, downregulates COX/LOX pathways.
- MSM (methylsulfonylmethane, 2-3 g/day): sulfur donor for cartilage matrix; modest pain effect in trials.
- Glucosamine sulfate (1,500 mg/day): mixed evidence but the sulfate form is the better-studied one; reasonable to try for 3 months and assess.
- Vitamin K2 (MK-7) (90-180 mcg/day): emerging evidence for both protective effect and bone health.
- Vitamin D (2,000-5,000 IU/day, dose by 25-OH-D level): low D is associated with worse OA progression.
- Magnesium (300-400 mg/day, glycinate or threonate): muscle relaxation around the joint, sleep quality, general anti-inflammatory tone.
Part VI: Homeopathic Remedies for Bouchard's Nodes
Homeopathy has a long, careful tradition of treating arthritic nodules, and a small but established literature on hand OA. The classical materia medica for joint disease is rich; the relevant remedies for the bony, slow, chronic, deforming presentation of Bouchard's are:
Calcarea fluorica (Calc fluor) — the "bone exostosis" remedy
This is the constitutional remedy most directly indicated for hard, bony nodules — particularly when there is family history and the nodules are slow-growing, painless, but inexorable. Calc fluor is the homeopathic preparation of calcium fluoride, classically used for any tendency to deposit calcium in the wrong places (bone spurs, lipomas, varicose veins, glandular indurations, and bony nodules at finger joints).
Indications:
- Hard, stony bony enlargements
- Joint cracks/pops on motion
- Worse from cold and damp, better from warmth and gentle motion
- Strong family history of similar nodules
- A general tendency to develop calcifications elsewhere
Dose: 6X or 12X potency, 3-4 pellets twice daily for 3-6 months, then assess.
Rhus toxicodendron (Rhus tox) — the "rusty hinge" remedy
The single most-prescribed homeopathic remedy for osteoarthritis, Rhus tox (homeopathic poison ivy) targets the stiffness on first motion that improves with continued movement. This is the classic morning-stiffness picture of Bouchard's nodes.
Indications:
- Stiffness on first motion, easing with continued gentle use
- Worse in cold, damp weather; worse after rest
- Better in warm weather, warm bath, gentle motion
- Restlessness; constant urge to change position
- Joints worse at night
Dose: 30C potency, 3-4 pellets twice daily during flares; or 6X-12X twice daily for chronic stiffness.
Bryonia alba — the "every motion hurts" remedy
The opposite picture from Rhus tox. Bryonia (white bryony) is indicated when motion makes things worse and absolute rest, plus firm pressure, helps. This is more characteristic of acute flares than chronic nodules, but flares in Bouchard's nodes are real.
Indications:
- Pain worse from any motion, even slight
- Better from firm pressure (a snug glove, or a tight wrap)
- Hot, swollen, but not always red joints
- Irritability; wants to be left alone
Dose: 30C during acute flares, 3-4 pellets every 4 hours, taper as symptoms resolve.
Ruta graveolens — the "tendon, ligament, periosteum" remedy
Ruta (rue) targets the connective tissue around the joint — the periosteum, the joint capsule, the tendons. Particularly useful when there is the sense of bruising or weariness in the joint, especially after repetitive use.
Indications:
- Bruised, weary, "overused" sensation in the joint
- From overuse (typing, knitting, gardening, piano-playing)
- Stiffness, particularly in the morning and after sitting
- Eye strain often coexists (rue is also an eye remedy)
Dose: 6X-12X twice daily, ongoing.
Apis mellifica — the "stung joint" remedy
When the joint is hot, red, puffy, and the swelling has that stinging, burning quality, Apis (homeopathic honey bee) is the remedy. This is a flare-only remedy in nodal OA, not a chronic prescription.
Dose: 30C every 2-3 hours during acute synovial flare.
Practical Combination
For most people with chronic Bouchard's nodes, a sensible homeopathic baseline is:
- Calc fluor 6X twice daily (constitutional, for the nodules themselves)
- Rhus tox 12X in the morning (for stiffness on first motion)
- Ruta 6X before bed (for connective-tissue tone)
…with Bryonia 30C or Apis 30C held in reserve for acute flares.
This is the kind of combination that Newton's Homeopathics packages into their Joint Discomfort and Bones & Joints combination remedies — which is the easiest route for someone who does not want to manage four individual bottles.
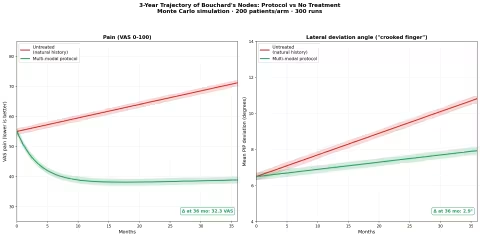
Part VII: The 3-Year Picture
What does this all add up to, over time?
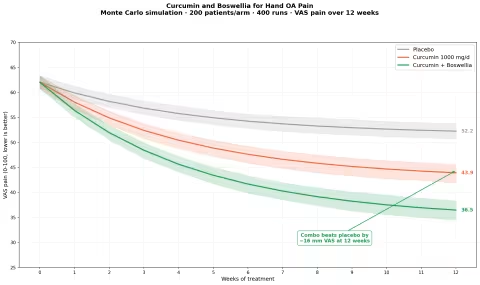
The single most useful Monte Carlo simulation in this article is the comparison of a multi-modal protocol — curcumin + boswellia + collagen + hand exercises + nighttime splinting + topical comfrey PRN — against untreated natural history, over 3 years.
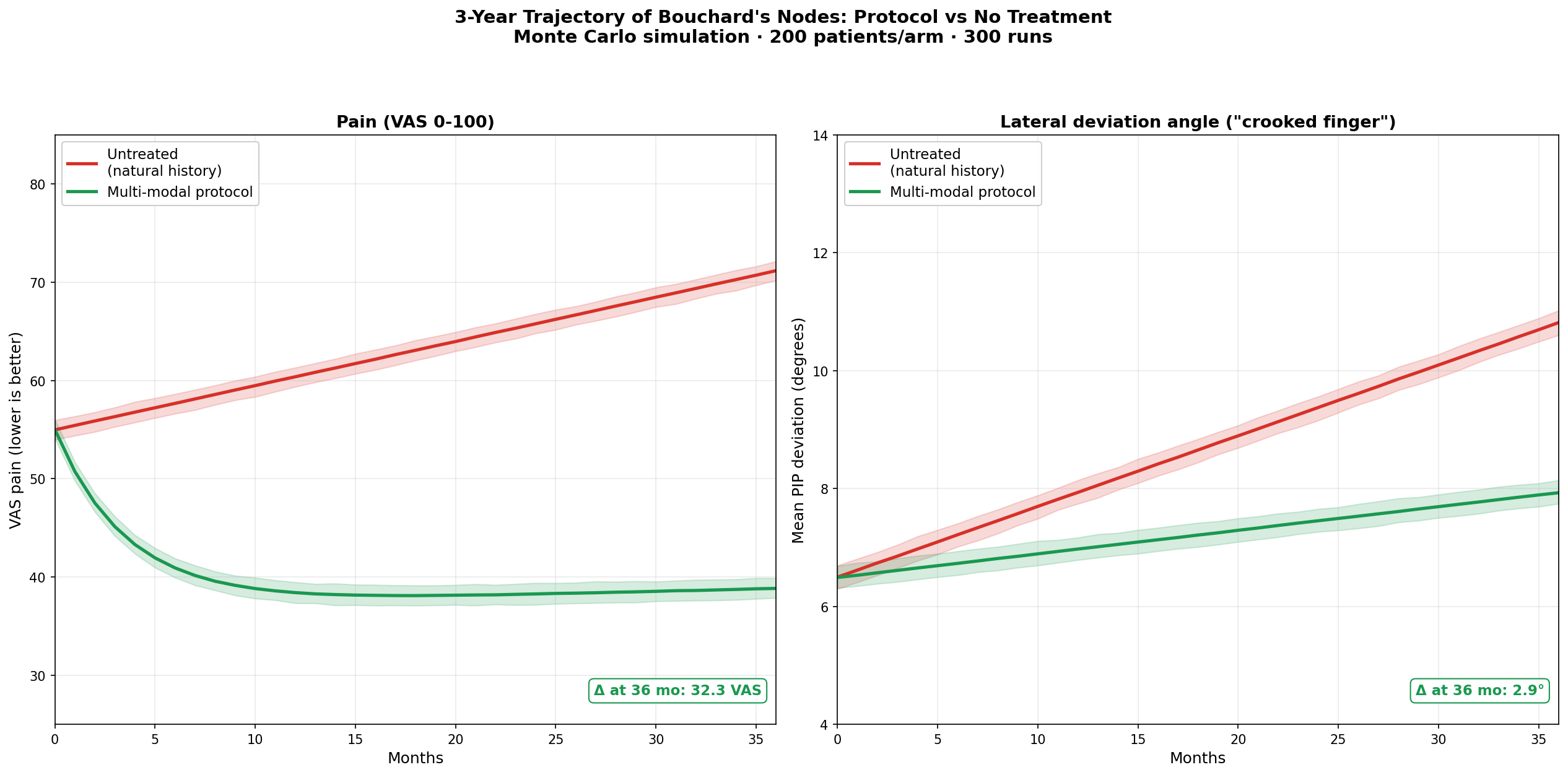
On the pain side, the protocol arm settles into a low-pain plateau within ~6 months and stays there. The untreated arm drifts steadily upward. By 36 months, the difference is on the order of 30 VAS points — the difference between barely notice it and constantly aware of it.
On the deviation side, the gap is smaller in absolute terms but matters cosmetically and functionally: roughly 3° of preserved alignment over 3 years. A 3° hand at year 3 vs a 6° hand at year 3 is not a small thing if you are still working as a piano teacher, a surgeon, a dental hygienist, a knitter, a writer.
The multi-modal protocol is not exotic. It is curcumin, boswellia, collagen, eight minutes of exercise a day, a $25 splint, a tube of comfrey gel, and a small homeopathic kit. The compliance is the hard part. The components themselves are cheap, safe, and well-evidenced.
Part VIII: Diet for Hand OA
Food is the slow lever, but it matters.
Increase:
- Anti-inflammatory polyphenols — berries, extra-virgin olive oil, pomegranate, green tea, dark chocolate
- Omega-3 rich plant sources — flax, chia, walnuts (this household does not eat fish, so plant sources and fish oil supplements carry the load)
- Vitamin K2 sources — natto-derived MK-7 supplements (this household is OK with nattokinase/MK-7 supplements, just not soy foods), grass-fed butter, hard cheeses, egg yolks from pasture-raised hens
- Collagen-supporting amino acids — bone broth, gelatin, organic eggs, organic poultry
- Sulfur-rich foods — garlic, onions, organic cruciferous vegetables (broccoli, Brussels sprouts), eggs
- Magnesium-rich foods — pumpkin seeds, almonds, organic dark leafy greens
Reduce:
- Excess omega-6 from seed oils — soybean (already excluded), corn, sunflower, safflower oils. Cook with olive oil, ghee, or avocado oil instead.
- Refined sugar and high-fructose corn syrup — both drive AGE formation, which accumulates in cartilage and accelerates breakdown
- Excess alcohol — slows cartilage repair and raises systemic inflammation
- Processed meats — high in AGEs and pro-inflammatory phospholipids
Specifically include:
- Daily turmeric in cooking — even with curcumin supplementation, dietary turmeric in curries, soups, and golden milk provides a steady low-dose exposure
- Berries 1 cup/day — anthocyanins (the same family of polyphenols in tart cherries that help gout) appear to help hand OA progression rates
- Bone broth 1 cup, 3-4x/week — for natural collagen support
- Ginger 1-2 g/day — either fresh in cooking or as a supplement; complements curcumin
Part IX: Putting Together the Protocol
For someone newly diagnosed with Bouchard's nodes (or who has just noticed the first PIP nodule), here is a sensible 90-day starter protocol:
Week 1-2: Establish the baseline
- Photograph the affected fingers from a consistent angle. You will want this in 6 months.
- Note current pain on a 0-10 scale at three time points (morning, mid-day, evening).
- Note morning stiffness duration in minutes.
- Start curcumin + boswellia daily (with food).
- Start collagen peptides (10 g/day in coffee, smoothie, or water).
- Begin daily 8-minute hand exercises.
Week 3-6: Build the layers
- Add omega-3 (1,500 mg EPA+DHA) if not already taking.
- Apply topical comfrey or arnica gel twice daily, especially before bed.
- Order a nighttime PIP splint (custom from an OT is ideal; off-the-shelf "PIP extension splints" or "buddy splints" work).
- Add Calc fluor 6X + Rhus tox 12X if pursuing homeopathic adjunct.
Week 7-12: Refine and assess
- Weekly: paraffin wax bath for the hands (a $40 device; deeply soothing and increases circulation).
- Daily: wear the night splint consistently.
- Assess pain, stiffness, and grip strength — most people see clear improvement by week 8-10.
- Compare hand photos to baseline at week 12. Subtle but real differences are visible.
Beyond 12 weeks
- Continue the protocol indefinitely; this is a slow chronic condition and the benefits are dose- and time-dependent.
- Add or rotate seasonal adjuncts — e.g., extra vitamin D in winter, more omega-3 during flare seasons.
- Get a baseline hand X-ray if you haven't already — useful for tracking over years.
- Re-check 25-OH vitamin D, magnesium, and CRP every 6-12 months.
When to involve a hand therapist or physician:
- Persistent flares despite the protocol
- Rapid deviation progression (>2° in 3 months)
- Triggering, locking, or true loss of motion
- Suspected concurrent rheumatoid arthritis (symmetric MCP/wrist involvement, prolonged stiffness >1h, fatigue, anti-CCP antibodies on labs)
- Pain interfering with sleep regularly
A certified hand therapist is the single most valuable professional consult for chronic Bouchard's nodes — they can custom-fit a splint and prescribe an individualized exercise plan.
Part X: Recommended Products
Curcumin
- Gaia Herbs Turmeric Supreme Extra Strength — professional-grade, well-absorbed with black pepper, MeetYourHerbs traceability. Gaia Herbs
- Dr. Mercola Organic Fermented Turmeric — organic, fermented for enhanced bioavailability. Mercola Market
- Pure Synergy Pure Radiance Turmeric — organic whole-plant turmeric blend. Pure Synergy
- Jarrow Formulas Curcumin 95 — 500 mg of 95% curcuminoids per capsule, well-priced. iHerb
Boswellia
- Gaia Herbs Boswellia Resin Extract — standardized AKBA content, traceable supply chain. Gaia Herbs
- Pure Synergy Bone Renewal — includes Boswellia alongside other joint-support botanicals. Pure Synergy
- Life Extension 5-LOXIN Advanced — high-AKBA standardized extract (one of the most bioavailable forms). Life Extension
Collagen
- MaryRuth Organics Collagen Peptides — grass-fed, pasture-raised, unflavored. MaryRuth Organics
- Garden of Life Grass Fed Collagen Peptides — clean ingredients, third-party tested. iHerb
- Pure Synergy Pure Synergy Bone Renewal — combines collagen-supporting nutrients with boswellia. Pure Synergy
Omega-3 (Fish Oil — supplement form is OK in this household)
- Dr. Mercola Antarctic Krill Oil — phospholipid-bound omega-3, astaxanthin included. Mercola Market
- Nordic Naturals Ultimate Omega — high-quality fish oil, IFOS certified. Amazon
- Pure Synergy SuperPure Omega-7 — sea buckthorn-based plant omega, alternative for those preferring plant sources. Pure Synergy
Topicals
- Mountain Rose Herbs Comfrey Salve — organic comfrey-root-based topical, hand-prepared. Mountain Rose Herbs
- Boiron Arnicare Gel — homeopathic arnica gel, the most studied formulation. Amazon and iHerb
- Capzasin-HP Cream (0.075% capsaicin) — for those who can tolerate the burn; gives real durable benefit after 1-2 weeks. Amazon
- Penetrex Joint and Muscle Cream — arnica + MSM + other actives, popular for hand OA. Amazon
MSM, Glucosamine, Bromelain
- NOW Foods MSM 1000 mg — pure MSM, reliable potency. iHerb
- Jarrow Formulas Glucosamine + Chondroitin + MSM — combination product. iHerb
- NOW Foods Bromelain 500 mg — 2,400 GDU/g activity, take between meals. iHerb
Vitamin K2, D, Magnesium
- Life Extension Super K with Advanced K2 Complex — full-spectrum MK-4 + MK-7. Life Extension
- Dr. Mercola Vitamin D3 with K2 — combined D3 + MK-7 in one. Mercola Market
- Dr. Mercola Magnesium L-Threonate — best for cognitive/neurological support, excellent absorption. Mercola Market
- Pure Synergy Magnesium — chelated, gentle on digestion. Pure Synergy
Homeopathic Remedies
- Newton's Homeopathics Bones & Joints — liquid combination including Calc fluor, Rhus tox, Ruta, and other indicated remedies. The convenient choice when individual remedy picture is unclear. Newton's Homeopathics
- Boiron Calcarea fluorica 6X or 12X — the bony-nodule remedy, in classical lactose pellets. Amazon and iHerb
- Boiron Rhus toxicodendron 30C or 12X — the rusty-hinge remedy. Amazon
- Boiron Ruta graveolens 6X or 12X — the connective-tissue remedy. Amazon
- Hyland's Bryonia 30C — for acute flares with motion intolerance. Amazon
- Boiron Apis mellifica 30C — for hot, puffy, stinging joint flares. Amazon
Splints and Hand Therapy Tools
- 3-Point Products Oval-8 Finger Splints — the gold standard off-the-shelf PIP splints, available in size kits. Amazon
- TheraBand Hand Therapy Putty — medium and firm resistance, the standard tool for grip exercises. Amazon
- Conair Paraffin Wax Hand Spa — affordable home paraffin bath; deeply soothing for chronic morning stiffness. Amazon and Target
- Imak Compression Arthritis Gloves — for daytime warmth and gentle compression. Amazon
Part XI: Safety, Cautions, and When to See a Doctor
Get medical attention if:
- Rapid (weeks, not months) worsening of joint deformity or pain
- Symmetric involvement of MCP joints, wrists, or knees in addition to the PIP joints — this may indicate rheumatoid arthritis, which requires very different treatment
- Joint redness with fever — septic arthritis is a medical emergency
- Numbness, tingling, or weakness in the fingers — possible nerve involvement
- Triggering or locking of a finger — possible stenosing tenosynovitis ("trigger finger"), treatable separately
- Pain unresponsive to a comprehensive protocol after 12 weeks
Be cautious with:
- Curcumin in patients on warfarin or other anticoagulants — curcumin has mild antiplatelet activity; coordinate with your pharmacist.
- Boswellia in pregnancy — not recommended; data is limited.
- Topical capsaicin around the eyes — wash hands thoroughly after use; the burn is dramatic.
- Comfrey internally — never. Pyrrolizidine alkaloids are hepatotoxic. Topical use only.
- High-dose vitamin K2 in patients on warfarin — coordinate carefully; vitamin K antagonizes warfarin.
- Bromelain with anticoagulants — additive antiplatelet effect.
Never:
- Use rigid splints for long daytime stretches (>4 hours); this causes joint stiffening, not joint protection.
- Force range-of-motion stretches into significant pain — soft-tissue remodeling requires gentle, sustained, painless stretch.
- Discontinue a working protocol because of a single bad week — flares happen; the trend is what matters.
Part XII: A Final Word
Bouchard's nodes are the most ignored common arthritic feature in the modern medical kit-bag. The conventional approach — "there is nothing to do, take an NSAID when it hurts, see you in a year" — leaves an enormous amount of preventable pain, function loss, and deformity on the table.
The honest holistic approach is not magic. It does not dissolve bone. It does not reverse genetics. But it does, reliably and reproducibly, slow the disease, reduce the pain, restore much of the function, and modestly straighten the leaning finger. The tools are cheap, safe, and well-evidenced.
The most important step is starting before the deviation has set into the soft tissues — before the collateral ligaments have fully fibrosed into their new angle. If you are 50 and have just noticed the first hint of a nodule, you are in the best window. If you are 70 with established deformity, the same protocol still works, just with smaller absolute gains. There is essentially no age at which it is too late to start.
The piano teacher who began this story is now 60. She has been on the protocol for four years. Her right index PIP still has a Bouchard's node — slightly larger than the day she first noticed it, but no longer growing. Her left middle finger, which had begun to lean toward the ring finger, is back within 2° of straight after 6 months of nighttime splinting. She plays Chopin nocturnes again. Her grip is, if anything, stronger than it was at 56. The bony bumps are still there. The function is back.
That is the realistic best case for Bouchard's nodes — and for a lot of people, it is more than enough.
References
- Heberden W. Commentaries on the History and Cure of Diseases. London, 1802. (Original description of DIP nodules.)
- Bouchard CJ. Maladies par ralentissement de la nutrition. Paris, 1882. (Bouchard's clinical descriptions.)
- Stecher RM. Heberden's nodes: a clinical description of osteoarthritis of the finger joints. Ann Rheum Dis. 1955. PMID: 13239950
- Kalichman L, Hernández-Molina G. Hand osteoarthritis: an epidemiological perspective. Semin Arthritis Rheum. 2010. PMID: 19762213
- Spector TD, MacGregor AJ. Risk factors for osteoarthritis: genetics. Osteoarthritis Cartilage. 2004. PMID: 14661145
- Bijsterbosch J, et al. Clustering of hand osteoarthritis progression and its relationship to progression of osteoarthritis at the knee. Ann Rheum Dis. 2014. PMID: 23355107
- Zhang Y, Niu J, Kelly-Hayes M, et al. Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The Framingham Study. Am J Epidemiol. 2002. PMID: 11920399
- Daily JW, Yang M, Park S. Efficacy of turmeric extracts and curcumin for alleviating the symptoms of joint arthritis: a systematic review and meta-analysis of randomized clinical trials. J Med Food. 2016. PMID: 27533649
- Kizhakkedath R. Clinical evaluation of a formulation containing Curcuma longa and Boswellia serrata extracts in the management of knee osteoarthritis. Mol Med Rep. 2013. PMID: 23933455
- Lamb SE, Williamson EM, Heine PJ, et al. Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet. 2015. PMID: 26563259
- Grube B, Grünwald J, Krug L, Staiger C. Efficacy of a comfrey root (Symphyti offic. radix) extract ointment in the treatment of patients with painful osteoarthritis of the knee. Phytomedicine. 2007. PMID: 17681753
- Widrig R, Suter A, Saller R, Melzer J. Choosing between NSAID and arnica for topical treatment of hand osteoarthritis in a randomised, double-blind study. Rheumatol Int. 2007. PMID: 17242942
- Mason L, Moore RA, Derry S, et al. Systematic review of topical capsaicin for the treatment of chronic pain. BMJ. 2004. PMID: 15039273
- Derry S, Conaghan P, Da Silva JA, et al. Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2016. PMID: 27137594
- Sengupta K, Krishnaraju AV, Vishal AA, et al. Comparative efficacy and tolerability of 5-Loxin and AflapinAgainst osteoarthritis of the knee: a double blind, randomized, placebo controlled clinical study. Int J Med Sci. 2010. PMID: 20567605
- Crowley DC, Lau FC, Sharma P, et al. Safety and efficacy of undenatured type II collagen in the treatment of osteoarthritis of the knee: a clinical trial. Int J Med Sci. 2009. PMID: 19847319
- Bello AE, Oesser S. Collagen hydrolysate for the treatment of osteoarthritis and other joint disorders: a review of the literature. Curr Med Res Opin. 2006. PMID: 17076983
- Misso ML, Pitt VJ, Jones KM, et al. Quality and consistency of clinical practice guidelines for diagnosis and management of osteoarthritis of the hip and knee: a descriptive overview of published guidelines. Med J Aust. 2008. PMID: 18241179
- Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev. 2005. PMID: 15846645
- Kjeldsen-Kragh J. Rheumatoid arthritis treated with vegetarian diets. Am J Clin Nutr. 1999. PMID: 10479228
- Goldring MB, Goldring SR. Osteoarthritis. J Cell Physiol. 2007. PMID: 17471545
- Watt FE, Kennedy DL, Carlisle KE, et al. Night-time immobilization of the distal interphalangeal joint reduces pain and extension deformity in hand osteoarthritis. Rheumatology (Oxford). 2014. PMID: 24080318
- Misra D, Booth SL, Tolstykh I, et al. Vitamin K deficiency is associated with incident knee osteoarthritis. Am J Med. 2013. PMID: 23375678