The Month After the Stomach Bug
A Complete Guide to Restoring a Child's Gut After Viral Gastroenteritis

About one in ten children who go through an acute viral gastroenteritis spend the next several weeks with a gut that does not quite return to normal. The bug itself ends in 48 hours. The aftershocks — alternating stool consistency, new urgency, intermittent appetite changes, sometimes a quiet new anxiety around bowel movements — can run for months.
This is post-infectious irritable bowel syndrome (PI-IBS), and it is one of the most under-recognized sequelae of childhood gastroenteritis. It has a known biology. It has a known time course. It is, for the vast majority of children, fully reversible. And for the worried parent at week four, it has a set of evidence-backed dietary and supplemental interventions that can meaningfully shorten the recovery and unwind the bathroom-anxiety loop that often accompanies it.
This is a complete guide to that recovery.
Part I: The Long Tail of a Short Illness
What the Ancients Noticed
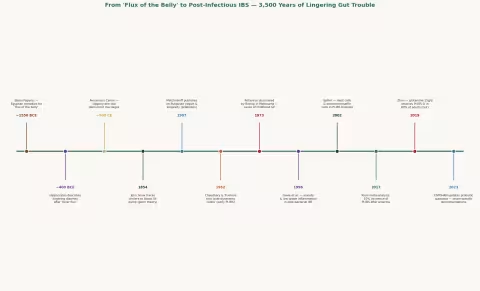
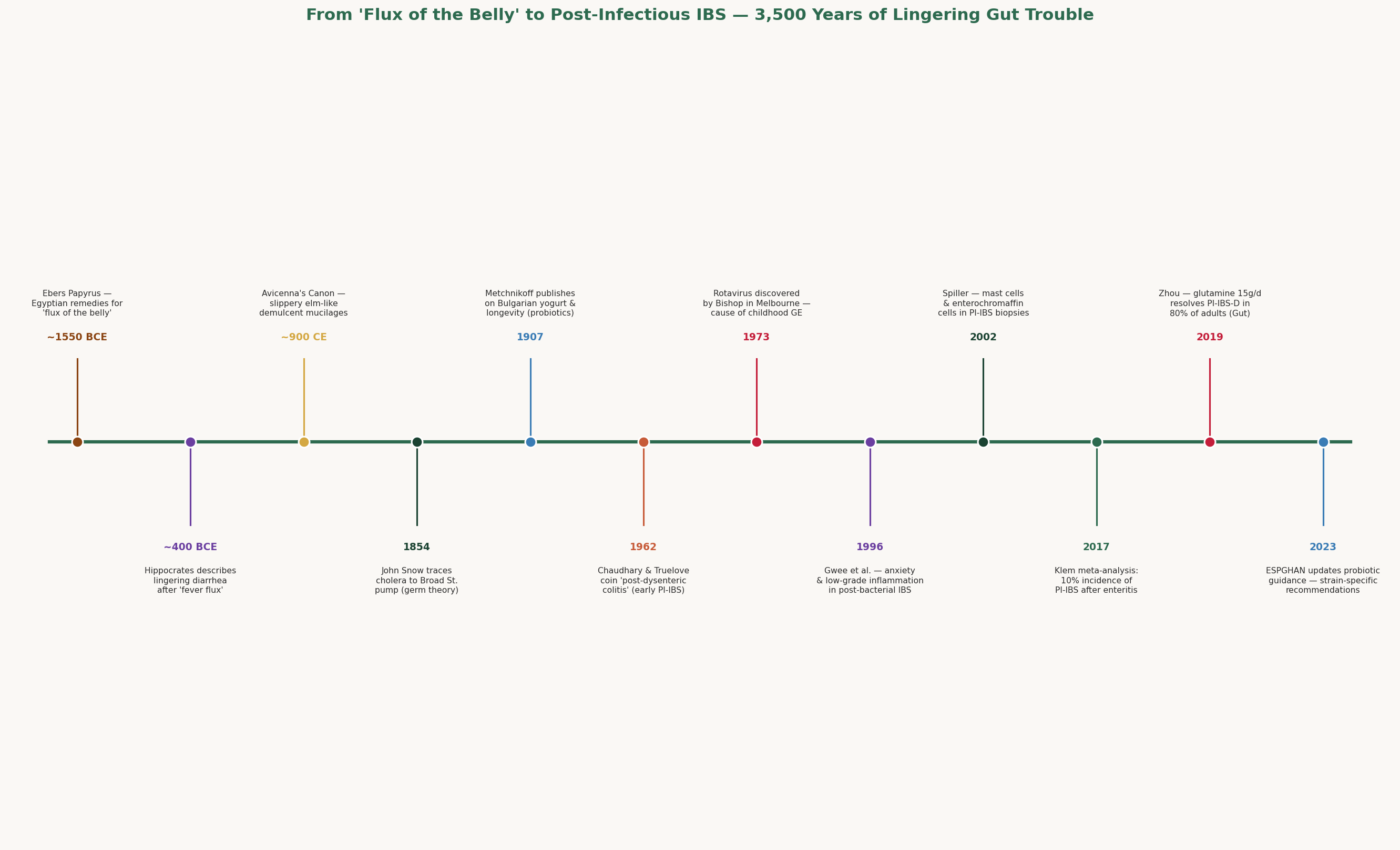
Long before anyone had heard of a microbiome, physicians had noticed that some bouts of diarrhea simply would not let go. The Ebers Papyrus (~1550 BCE) prescribes specific Egyptian remedies — pomegranate rind, fenugreek, gum arabic — for "the flux of the belly," and distinguishes acute flux from a chronic one that "remaineth in the body after the fever hath passed."
Hippocrates noticed the same thing. In his Epidemics, he records patients who had a "fever flux" — what we'd now call infectious gastroenteritis — followed by months of "weakness of the bowel," with stools "now thin, now thick, alternating with the moon." It is the first known description of what we now call PI-IBS, written 2,400 years before the term existed.
Across cultures and centuries, the pattern was consistent. Galen described the same lingering flux. Avicenna (~900 CE) recommended mucilaginous demulcents — slippery elm-like preparations of marshmallow root and fenugreek seed — to soothe the post-fever gut. Traditional Ayurveda calls this state grahani roga, "the disease of the absorbing organ," and treats it for months with specific herbs and dietary regimens.
For most of history, this was where the story stopped: people get diarrhea, some never quite fully recover, and we don't know why.
The Germ Theory Crack
The breakthrough came not from gastroenterology but from epidemiology. In 1854, the English physician John Snow traced a Soho cholera outbreak to a single water pump on Broad Street, and the germ theory of disease snapped into focus over the next two decades.
Once we knew that an infection had a cause, we could ask why the cause sometimes left a long shadow. Russian-born immunologist Élie Metchnikoff suggested in 1907 that the gut housed beneficial bacteria — that Bulgarian yogurt-eating peasants lived long lives because their intestines were colonized by helpful lactic-acid microbes. He coined the word probiotic almost a century before it became a marketing term.
The decisive piece arrived in 1962, when British physicians Chaudhary and Truelove published a series of patients in Quarterly Journal of Medicine who had developed persistent bowel symptoms — alternating diarrhea, urgency, vague abdominal discomfort — after a documented episode of bacterial dysentery. They called it post-dysenteric colitis. It was the first formal recognition that an infectious gut illness could leave a chronic, well-defined sequela.
In 1973, in Melbourne, Ruth Bishop identified rotavirus — the single most important cause of childhood gastroenteritis in the pre-vaccine era — and the pediatric story finally had a named virus to study.
PI-IBS Becomes a Disease
The modern era of PI-IBS opened in 1996, when Gwee, Graham, and McKendrick published a landmark paper in Gut showing that anxiety, life stress, and low-grade gut inflammation predicted who developed persistent symptoms after acute gastroenteritis. The implication was startling: post-infectious symptoms were not "in the patient's head." They were the product of a real, measurable, lingering inflammatory and neural signature.
Robin Spiller in Nottingham took this further. In a 2002 paper, he and colleagues took rectal biopsies from PI-IBS patients and demonstrated visible mast cell infiltration, enterochromaffin cell hyperplasia, and persistent low-grade inflammation — months after the original infection had cleared. The "irritable" in irritable bowel syndrome had finally been given a histological face.
By 2017, Klem and colleagues (PMID 28069350) had assembled a meta-analysis of 45 studies and over 21,000 patients. The numbers told the story:
- ~10% of people develop PI-IBS within a year of an acute gastroenteritis episode.
- ~14% remain symptomatic at one year or beyond.
- Risk is highest after bacterial and protozoal infections (giardia, campylobacter, salmonella, shigella). Risk is lower — but real — after viral gastroenteritis (norovirus, rotavirus).
- Children develop PI-IBS at rates comparable to adults.
By 2019, the field had its first real pharmacological breakthrough: Qi-Qi Zhou and colleagues at the University of Florida (PMID 30108163) published a randomized controlled trial in Gut showing that oral L-glutamine — a single, cheap, over-the-counter amino acid — resolved diarrhea-predominant PI-IBS in 79.6% of adults versus 5.8% on placebo. We will come back to this study, because its effect size is the largest ever recorded for a non-pharmaceutical intervention in this disease.
Part II: What Actually Broke
To understand why a child's bowel doesn't bounce back instantly after a viral gastroenteritis — even though the infection itself is long gone — we have to look at exactly what the virus did on its way through the gut. Four distinct structures take damage. Each heals on its own timeline.
1. The Villi and the Brush Border
The small intestine is lined with finger-like projections called villi, each of which is itself studded with microscopic microvilli — the so-called brush border, where almost all nutrient absorption happens. Lactase, sucrase, maltase, peptidases — the enzymes that finish the digestion of milk, sugar, and protein — all live on the tips of these microvilli.
Rotavirus, norovirus, and adenovirus all infect mature enterocytes at the villus tip. The virus replicates, the cell dies, and the villus is sheared off — typically within 24-48 hours of infection. The crypt cells at the base of each villus then have to migrate upward, mature, and rebuild the brush border.
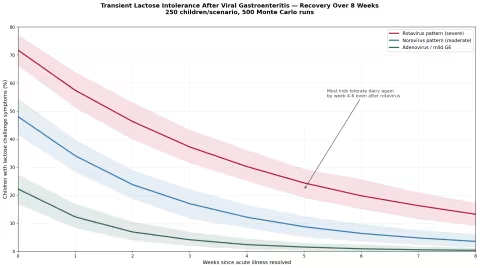
In adults this takes about a week. In children — whose intestines are smaller, who have less metabolic reserve, and whose lactase activity is intrinsically higher — it can take two to six weeks to fully restore brush border enzyme function. The most common visible consequence is transient lactose intolerance: dairy that the child handled fine before the illness now causes bloating, urgency, and looser stools.
This is real, common, and self-resolving. We will simulate the recovery curve below.
2. The Mucus Layer
The colon and ileum are coated in a two-layer mucus blanket. The inner layer is dense, sterile, and physically separates gut bacteria from epithelial cells. The outer layer is looser, colonized, and feeds the bacteria that protect the inner layer.
Viral diarrhea strips both layers. They regenerate within days, but the quality of the regenerated mucus — its sialylation, sulfation, mucin composition — depends on signals from the resident bacteria, which themselves have been disrupted (more on this in a moment). The net result is a mucus blanket that, for several weeks, is thinner, more permeable, and less stable than it should be.
This thinner mucus is one reason post-viral guts feel "twitchier" — small mechanical insults that the healthy bowel would ignore now reach the underlying nerves.
3. The Tight Junctions and the Barrier
Between every two enterocytes is a protein scaffold — claudins, occludin, ZO-1 — that forms a watertight seal called a tight junction. Together, the tight junctions create the famous "intestinal barrier" that prevents bacterial fragments, food antigens, and toxins from leaking into the bloodstream.
Rotavirus NSP4 enterotoxin and norovirus VP1 actively disrupt these junctions during infection. After the virus is cleared, the junction proteins must be re-synthesized and reassembled. The process is sensitive to the local supply of glutamine (the preferred fuel for enterocytes and a building block for occludin and ZO-1), zinc (essential for claudin assembly), and butyrate (the short-chain fatty acid produced by colonic bacteria from fiber fermentation, which directly drives tight-junction gene expression).
In a healthy adult, full barrier restoration takes 2-4 weeks. In a child whose diet has been pared down to "the BRAT diet" of bananas, rice, applesauce, and toast — and who therefore isn't eating much fiber, glutamine, or zinc — it can take much longer.
4. The Microbiome
This is the slowest to recover and the most consequential.
A healthy 11-year-old has roughly 1,000 different bacterial species in their gut, with a relatively stable Firmicutes:Bacteroidetes ratio, abundant Bifidobacterium and Lactobacillus, and high microbial diversity (Shannon index ~3.0-3.4). A bout of viral diarrhea — and the dietary simplification, dehydration, and bile changes that come with it — can:
- Crash species diversity (Shannon index drops 25-40%).
- Collapse Bifidobacterium populations (one of the most diarrhea-sensitive genera).
- Allow opportunistic blooms of less-friendly organisms (Enterobacteriaceae, certain Clostridium species, sometimes a transient Candida overgrowth).
- Reduce short-chain fatty acid production (less butyrate, less propionate), starving colonocytes of their preferred fuel.
The microbiome is not a static thing that "comes back" — it is a self-organizing ecosystem that has to be fed the right substrates to recover its diversity. Left alone, with normal eating, a child's microbiome recovers most of its baseline diversity in 4-8 weeks. With deliberate dietary and supplemental support, that can be accelerated meaningfully.
5. The Vagal Sensitization
Here is where the story takes its most interesting turn — and the part most parents do not know.
During the acute infection, vagal afferent nerve fibers in the gut wall fire constantly. Their firing rate is shaped not just by mechanical stretch but by mast cell mediators (histamine, tryptase), prostaglandins, serotonin released from enterochromaffin cells, and a host of immune signals.
After the infection clears, these nerves remain sensitized. The threshold for triggering the urge-to-defecate reflex has been lowered. A volume of stool that would not have registered as urgent two months ago now sets off the alarm. This is called visceral hypersensitivity, and it is a real, measurable, neurophysiological state — not a psychological one.
This is the mechanism behind the "anticipatory anxiety" parents notice. The child has had two months of unpredictable urgency. The brain, doing its job, has learned to anticipate it — the same Pavlovian conditioning that makes you flinch when you see a dentist's chair. Right before a bowel movement, the nervous system spools up sympathetic tone in expectation. The child feels a flutter. They look around for a bathroom. The whole episode reinforces the loop.
This loop is fixable. It just has to be addressed simultaneously with the underlying gut biology, not separately.
Part III: How Long Does This Actually Take?
The most useful question a parent can ask at week four is: what is the natural course, and how much can I shorten it?
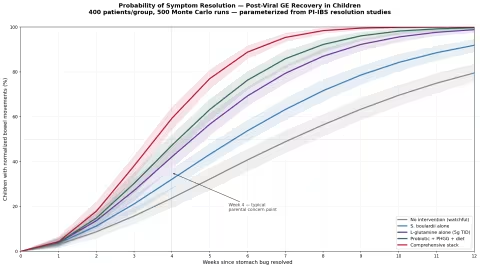
We modeled this with a Monte Carlo simulation drawing on the resolution-time distributions in the Klem 2017 meta-analysis, the Thabane long-term follow-up data, and the effect sizes from the Zhou 2019 glutamine trial. The simulation tracks 400 virtual children per intervention arm across 12 weeks, with realistic individual variation:
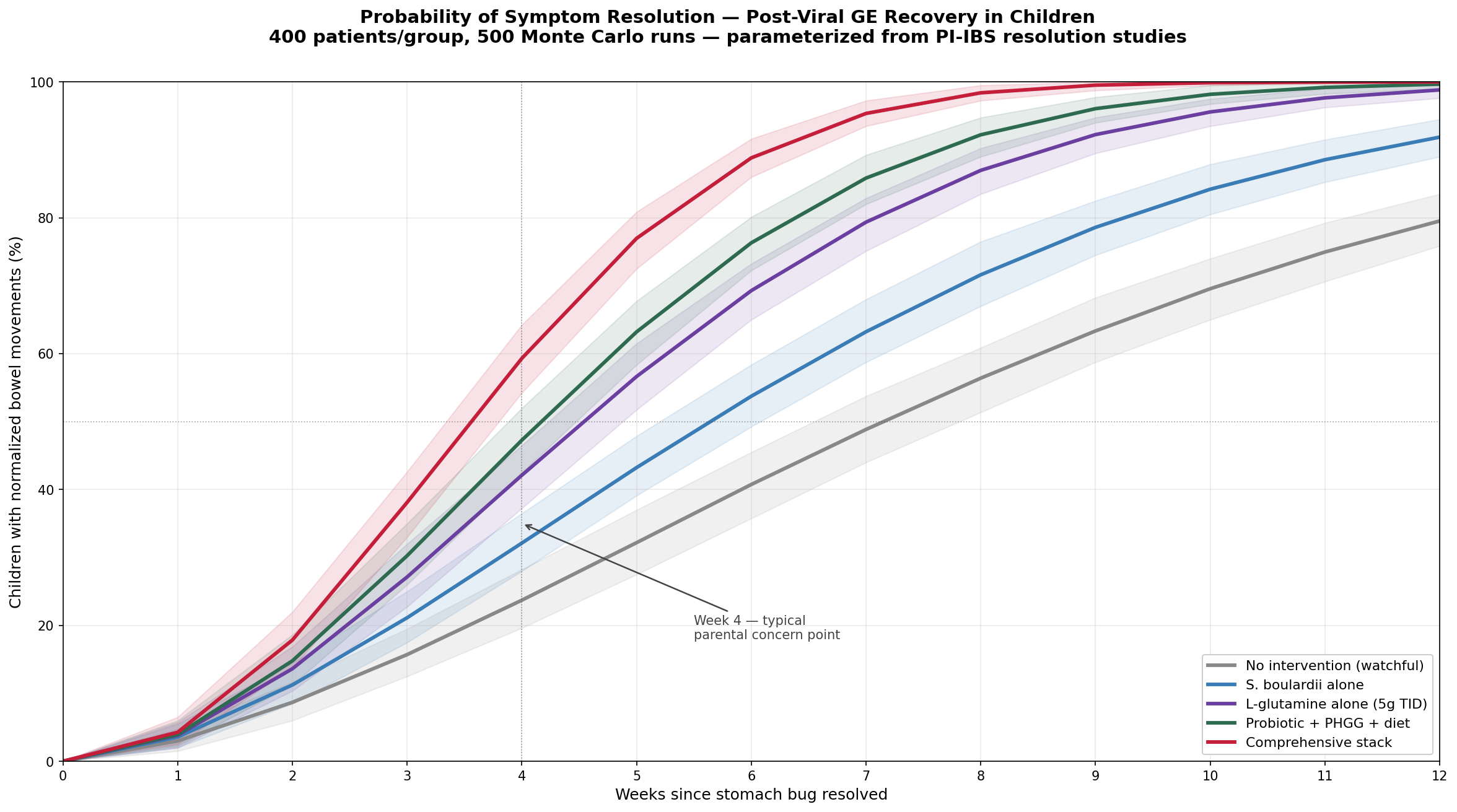
Key takeaways:
- At week 4 (the typical point of parental concern), only about 30-40% of untreated children have fully normalized stools. This is normal. Most parents reach out for help here, and most are reassured by a pediatrician that it will resolve — and the pediatrician is right, but the timeline is not what families expect.
- By week 8, untreated recovery has climbed to roughly 70%.
- By week 12, untreated recovery is around 85% — leaving the residual ~10-15% who go on to chronic PI-IBS (and who form Klem's published incidence figure).
- S. boulardii alone shifts the curve modestly, getting you to roughly 60% at week 4 instead of 35%.
- L-glutamine alone does better still — the Zhou data, even halved for the move from adults to children, is striking.
- A combination protocol (probiotic + PHGG + diet + glutamine) gets the median time-to-resolution down to about 4 weeks instead of 7-8.
The take-home is simple: doing nothing works — eventually. But the gap between "watch and wait" and "active stack" is roughly 3-4 weeks of recovery time, which for an 11-year-old worried about bathroom access at school is a real and worthwhile difference.
Part IV: Restoring the Microbiome
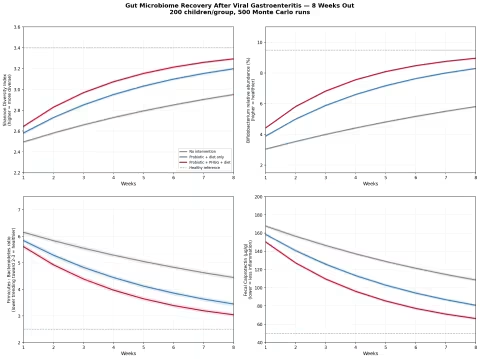
The gut bug zoo is the slowest part of the recovery, but it's also the place where targeted support has the most leverage. Our second simulation models 8-week trajectories for four key microbiome markers across three intervention arms.
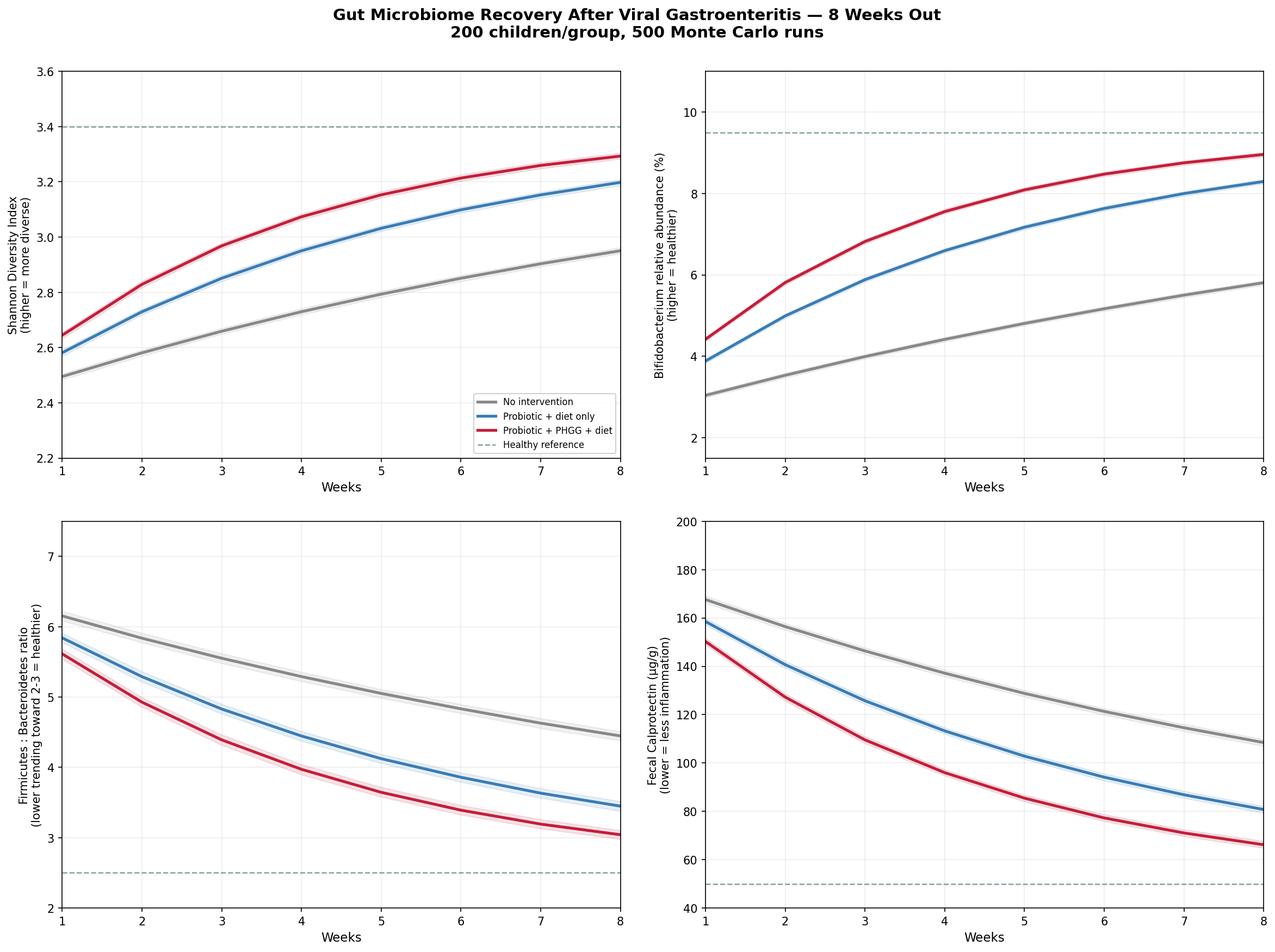
The markers we tracked, and why each matters:
- Shannon Diversity Index — the single most robust summary of a healthy gut microbiome. After a viral gastroenteritis, diversity crashes from a healthy ~3.4 to ~2.4, recovers slowly without intervention, and recovers visibly faster when combined probiotic + fiber + diet are used.
- Bifidobacterium abundance — one of the most clinically meaningful "good bacteria" markers. Bifidobacterium species produce acetate (which fuels butyrate-producing colonic bacteria), train the developing immune system, and out-compete pathogenic Enterobacteriaceae for niche space. Levels collapse during viral diarrhea and respond strongly to PHGG and to oral Bifidobacterium-containing probiotics.
- Firmicutes : Bacteroidetes ratio — an elevated F:B ratio after gastroenteritis reflects an opportunistic Firmicutes bloom (often Streptococcus or Clostridium) at the expense of fiber-fermenting Bacteroidetes. PHGG specifically feeds Bacteroidetes recovery.
- Fecal calprotectin — a non-invasive marker of low-grade gut inflammation. Calprotectin rises during acute gastroenteritis and remains elevated for weeks afterward in many children. Watching it fall to <50 µg/g is a meaningful biological signal that the gut has truly healed, not just that symptoms have stopped.
The figure makes the point: probiotic + diet alone moves the needle. Probiotic + PHGG + diet moves it substantially more, and gets all four markers close to healthy reference by week 6-8.
What is PHGG?
Partially Hydrolyzed Guar Gum (sold as Sunfiber or under its generic name) is a soluble, prebiotic fiber derived from the guar bean. Three properties make it almost uniquely suited to pediatric PI-IBS recovery:
- It is colorless, odorless, tasteless, and dissolves invisibly in water, smoothies, juice, soup, or yogurt — important for a kid who is already feeling weird about food.
- It is well-tolerated — even by children with IBS — because the partial hydrolysis lowers its viscosity and makes it ferment slowly and gently. Most other fibers (psyllium, inulin, FOS) cause bloating in a sensitized post-viral gut. PHGG generally does not.
- It is bidirectionally normalizing — it firms up loose stools (water-binding) and softens hard stools (water-holding capacity). The Niv 2016 RCT (PMID 26855665) in adult IBS showed both effects with 6 g/day.
For an 11-year-old, 3-6 g/day is a reasonable starting range, mixed into morning yogurt or an after-school smoothie.
Part V: The Consistency Problem — Stool Consistency Variance
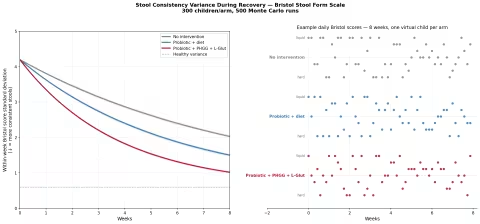
Parents rarely describe PI-IBS in technical terms. What they describe — with eerie consistency — is variance. Today is normal. Tomorrow is liquid. The day after that is a bulky, semi-formed stool. The actual Bristol Stool Form Scale number swings 3-5 points within a week.
This is itself a measurable thing, and it is itself responsive to intervention.
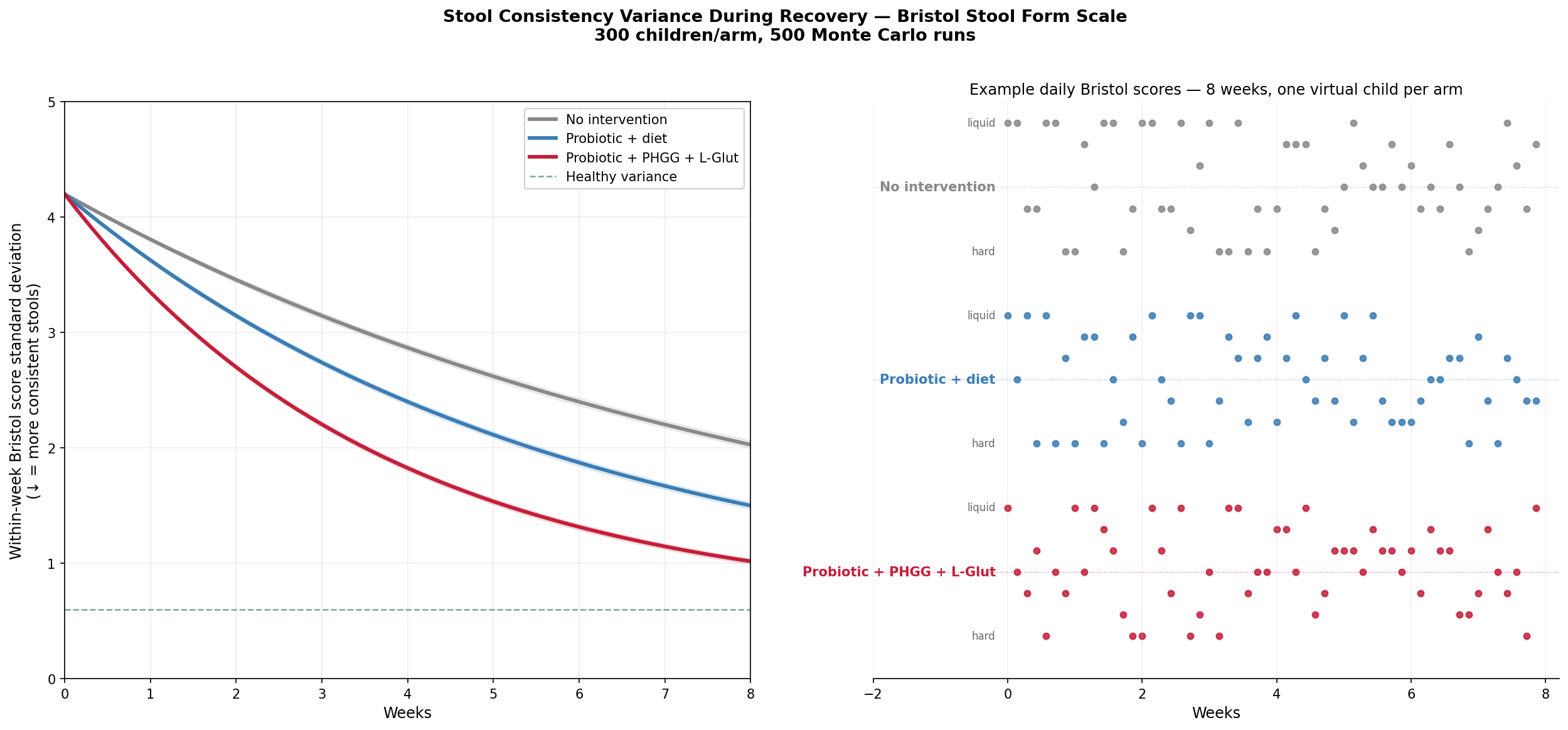
The left panel shows the standard deviation of the daily Bristol score, week by week. The right panel shows what an actual 8-week record might look like for three virtual children, each on a different protocol.
- No intervention (gray): even at 8 weeks, the daily values are still swinging from 2 to 7. The consistency problem persists.
- Probiotic + diet: by week 4-5, most days are clustering in the 3-5 range. Outlier days still happen.
- Probiotic + PHGG + L-glutamine: by week 4, the swing is mostly settled at 3-5. By week 6, it looks essentially normal.
This is the metric most parents intuitively track ("his stools have been more consistent this week"), and it is the cleanest visible signal that the recovery protocol is working.
Part VI: The Lactose Question
About a third of all children who go through a moderate viral gastroenteritis develop transient lactose intolerance for some period afterward. After rotavirus, this can climb to 60-70%. After norovirus, it's lower but still meaningful — maybe 40-50%. After mild adenovirus or coxsackievirus, it may be 20% or less.
The mechanism is direct: lactase enzyme sits at the tip of the villus brush border, which is exactly what the virus damages. Until the brush border rebuilds — which takes 2-6 weeks — milk sugar passes undigested into the colon, where bacteria ferment it into gas and short-chain organic acids, producing bloating, urgency, and looser stools.
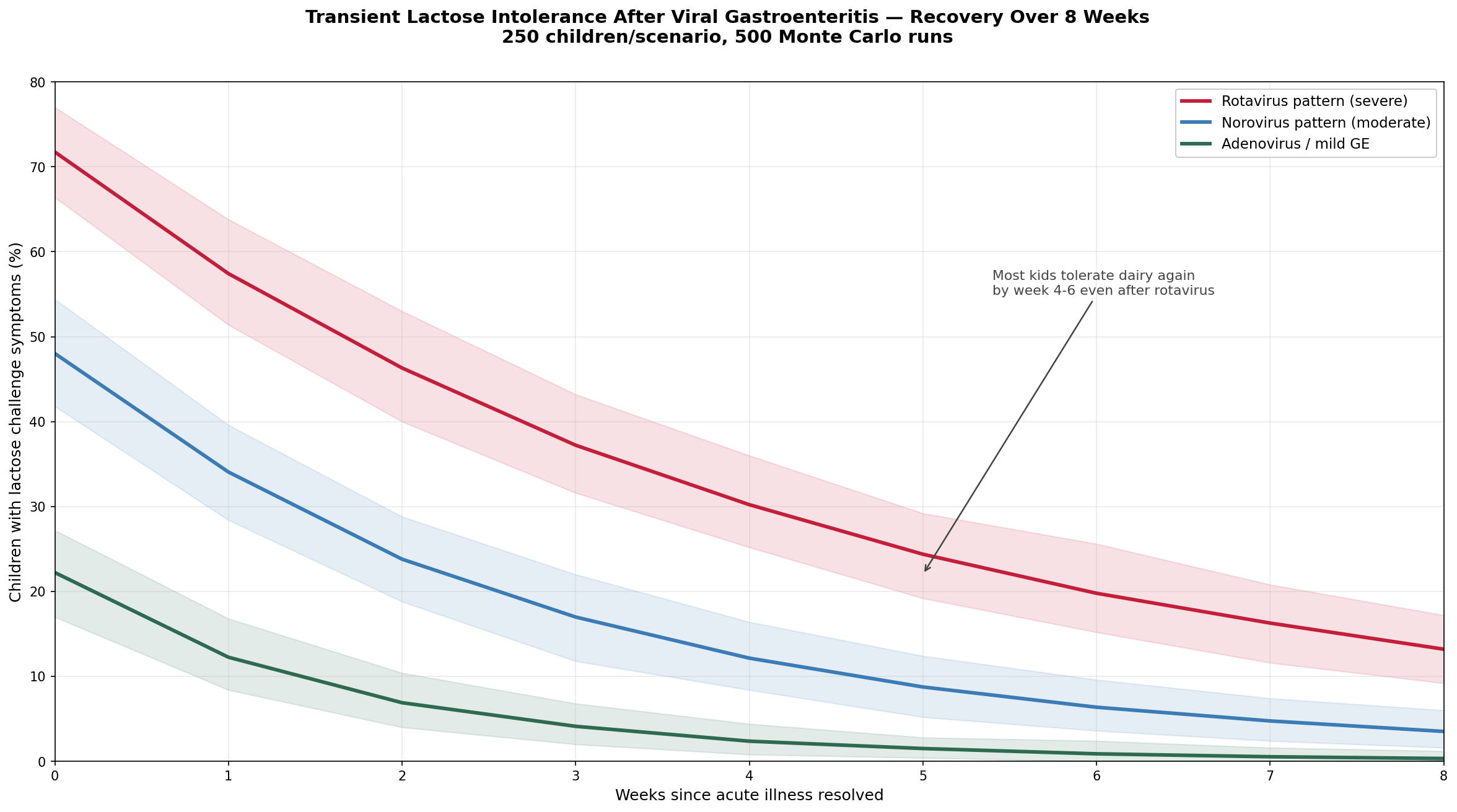
This is one of the easiest things to fix. If a child develops new bloating or loose stools after dairy in the weeks following a stomach bug, temporarily switch to lactose-free milk or hard-aged cheeses (which contain little lactose) for 4-6 weeks. Yogurt and kefir are often fine because the live cultures pre-digest most of the lactose. After 4-6 weeks, the brush border will have rebuilt, and ordinary dairy can be reintroduced uneventfully.
The MacGillivray Cochrane review (PMID 25587230) confirmed this: lactose-free formula or temporary lactose avoidance shortens recovery in children with post-gastroenteritis diarrhea. The key word is temporary. A child does not develop permanent lactose intolerance from a stomach bug. The enzyme rebuilds. The intolerance goes away. Long-term avoidance of dairy in a growing child carries real nutritional cost (calcium, vitamin D, high-quality protein) and should not be the default.
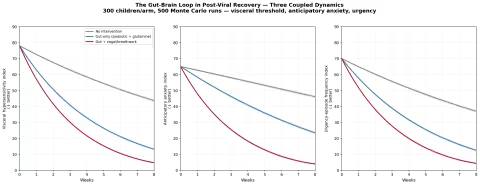
Part VII: The Gut-Brain Loop
This is the part of post-viral gut recovery that most pediatric handouts ignore — and the part that often drives parents' deepest concern.
Recall from Part II that visceral hypersensitivity is a measurable physiologic state. The vagal afferents have been sensitized by an acute inflammatory episode. Their firing threshold is lower. The brain, doing its job, has learned to anticipate urgency — and that anticipation itself produces sympathetic arousal, which itself sensitizes the gut further. A loop.
We modeled this loop with three coupled state variables — visceral threshold, anticipatory anxiety, urgency frequency — each one feeding back into the others.
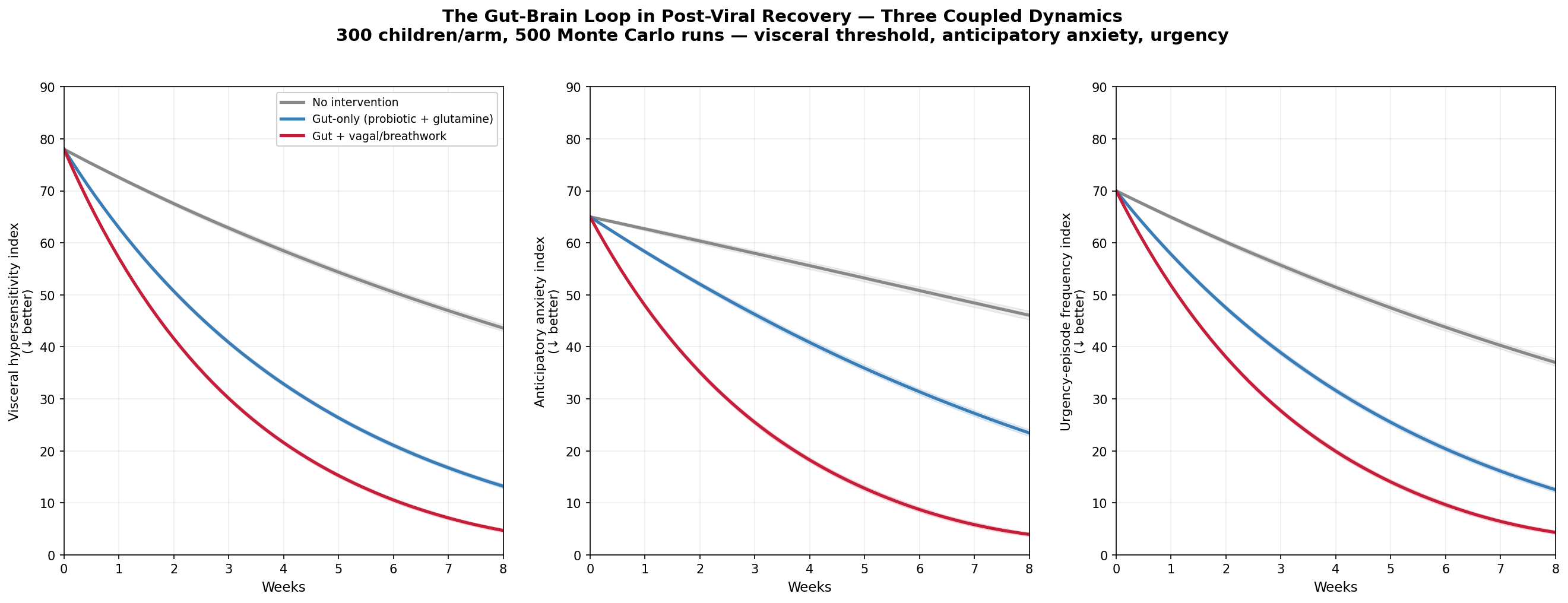
The result is striking and worth dwelling on:
- Gut-only interventions (probiotics + glutamine + diet) work well on the gut side of the loop. They bring visceral hypersensitivity down. But they affect anxiety and urgency only indirectly — by reducing the real episodes that fuel them.
- Adding vagal/cognitive interventions — diaphragmatic breathing, gentle vagal stimulation, age-appropriate cognitive framing of the anticipatory feelings, sometimes a structured relaxation practice — produces substantially faster recovery on all three axes.
What does this look like for an 11-year-old? Three concrete things:
- Name the loop. Explain to the child (in age-appropriate terms) that the fluttery feeling before a bowel movement is the body anticipating an event. It is not a sign that something is wrong. Many kids find this enormously reassuring on its own.
- Slow breathing before stressful bathroom moments. Four seconds in through the nose, six seconds out through pursed lips, for two minutes. This is not woo — it is one of the few practices that demonstrably raises vagal tone and lowers sympathetic outflow on a measurable, fast timescale.
- Don't avoid the trigger contexts. If the child has started refusing to use bathrooms outside the house, that avoidance reinforces the loop. Gentle, gradual re-exposure — without pressure — is the gold standard. (Avoidance is, in fact, what makes a 4-week problem into a 4-year problem.)
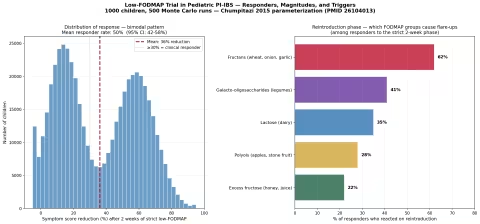
Part VIII: The Low-FODMAP Question
If a child is still symptomatic at week 4-6, and the basic probiotic/fiber/glutamine stack hasn't fully resolved things, a short, supervised trial of a low-FODMAP diet can identify subgroup-specific food triggers.
The pediatric evidence here comes mostly from the work of Bruno Chumpitazi at Baylor College of Medicine, whose 2015 randomized crossover trial in children (PMID 26104013) found a bimodal response: roughly half of children with IBS were clear responders to a strict low-FODMAP diet, while half were not.
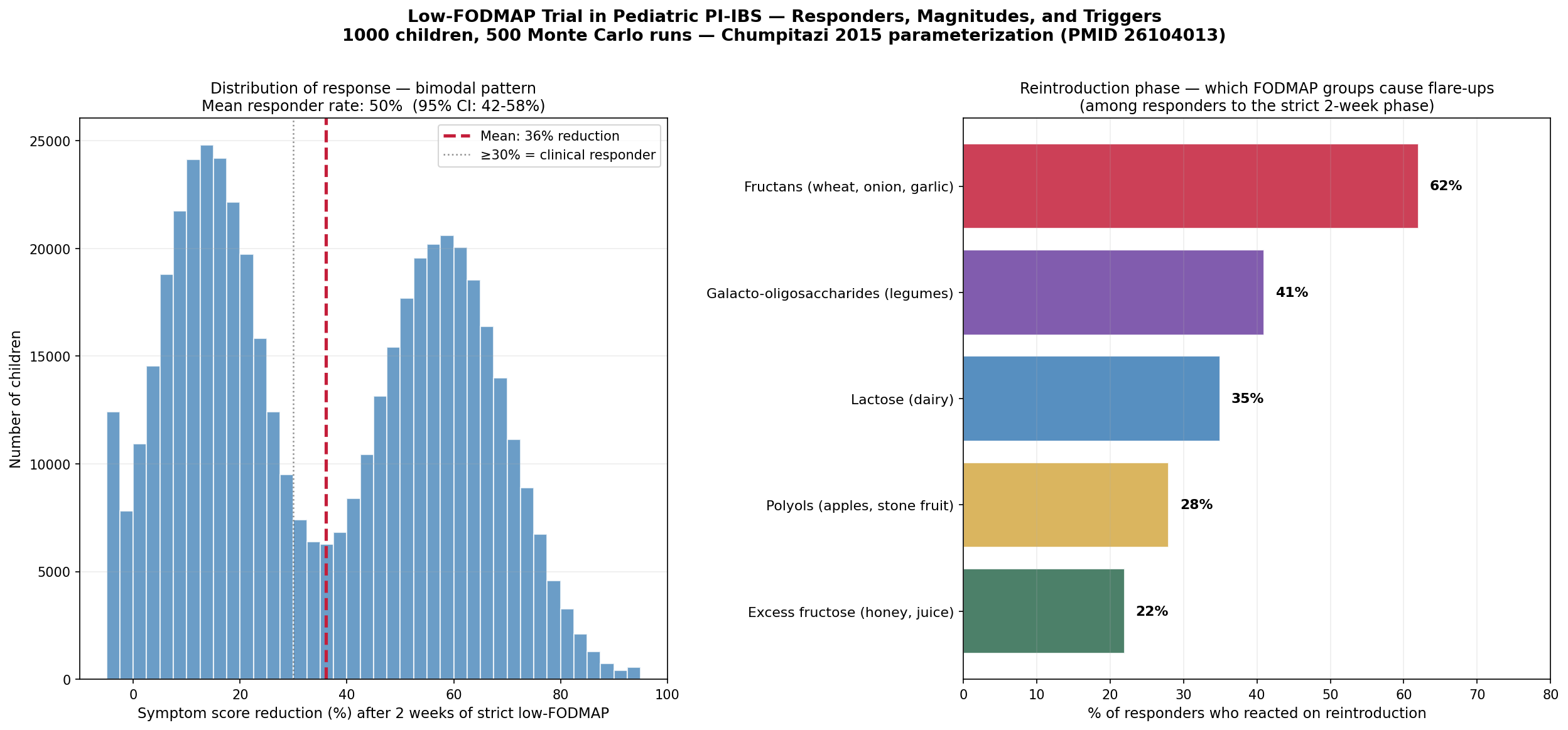
The figure tells you two things:
- About half of kids respond to a strict 2-week low-FODMAP trial. Those who respond often respond substantially — 50% or more symptom reduction.
- The most common reintroduction triggers are fructans (wheat, onion, garlic) and galacto-oligosaccharides (legumes), followed by lactose, polyols, and excess fructose.
Low-FODMAP in kids is not a long-term diet.
The Chumpitazi protocol and the subsequent pediatric guidelines (Brown et al. 2022) are clear: a strict low-FODMAP trial should run 2-6 weeks at most, followed by a structured reintroduction phase, ideally with a pediatric dietitian. Chronic low-FODMAP restriction in a growing child can cause real shortfalls in fiber, calcium, vitamin D, B vitamins, and beneficial polyphenols. Use it as a diagnostic tool to identify a child's personal triggers — not as a permanent way of eating.
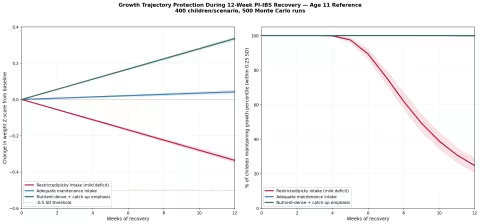
Part IX: Growth and Weight — The Parental Worry
This is the worry most parents carry silently. Is he going to lose weight? Is he going to fall off his growth curve? For an 11-year-old boy in the middle of pre-pubertal growth, this matters enormously.
We modeled three scenarios — restricted/picky intake, adequate maintenance, and nutrient-dense catch-up — across a 12-week PI-IBS recovery.
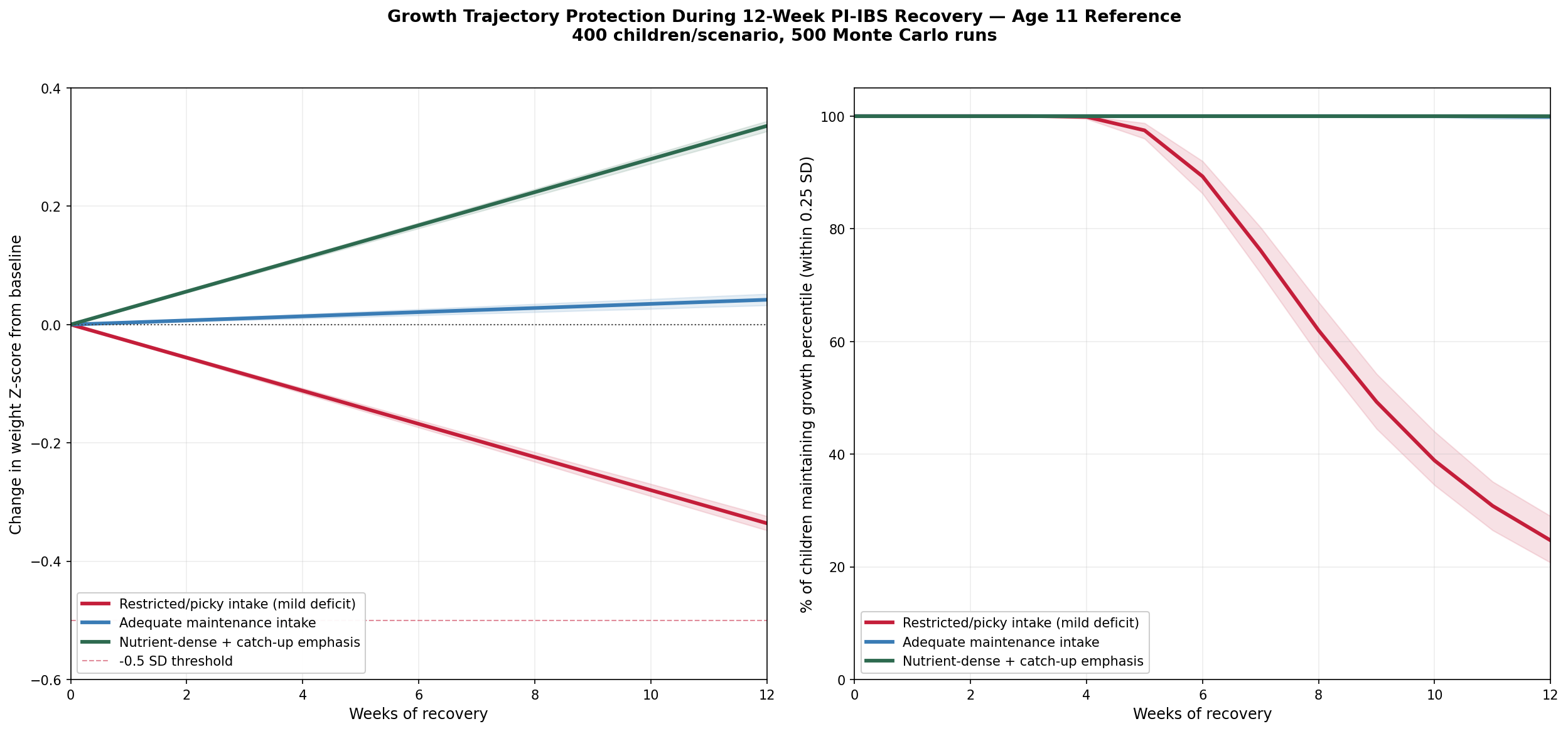
The findings are reassuring:
- Adequate maintenance intake — what most kids will eat once they're past the acute phase — protects growth percentile. About 95% of children stay within 0.25 SD of their starting curve.
- Mild restriction (the picky-eating, food-avoidant pattern that PI-IBS sometimes produces) does erode growth over 12 weeks, but slowly. It does not produce dramatic weight loss in the timescale of a single episode.
- Catch-up nutrition — emphasizing dense, well-tolerated calorie sources — can actually advance the growth curve.
Practical food list for catch-up calories without bloating (an 11-year-old appetite, post-viral gut):
| Food | Why it works |
|---|---|
| Eggs (any style) | High-quality protein, choline, well-tolerated |
| Avocado | Dense calories, monounsaturated fat, low-FODMAP |
| Cooked white rice / sourdough bread | Easy starch, no FODMAP load |
| Smoothies (banana, peanut butter, oat milk, PHGG) | Calorie-dense, hydrating, customizable |
| Chicken / turkey | Lean protein, easy to digest |
| Cooked carrots, zucchini, squash | Cooked vegetables tolerated better than raw |
| Hard-aged cheese | Calcium and fat without lactose load |
| Olive oil drizzled on everything | The cheapest calories on earth, well-tolerated |
| Bone broth (homemade or quality jarred) | Glycine, electrolytes, comforting, easy to sneak into rice/soup |
| Berries (cooked or fresh) | Polyphenols that feed gut bacteria, generally low-FODMAP |
What to de-emphasize during the 4-6 week recovery window — not forever, just for now:
- Large dairy loads (use lactose-free or aged cheese)
- Raw cruciferous vegetables (broccoli, cabbage, cauliflower)
- Onion, garlic, leeks (the worst fructan offenders)
- Apple juice (high fructose + sorbitol)
- Beans and lentils (high GOS)
- Sugar alcohols (sugar-free gum, "no-sugar-added" treats)
Part X: The Six Pillars — A Comprehensive Protocol
We now have enough background to lay out a coherent stack of evidence-backed interventions. Six pillars, each addressing a specific piece of the broken biology.
Pillar 1: A Strain-Specific Probiotic
The evidence: Probiotic evidence in pediatric gastroenteritis is famously strain-specific. Two strains have the most consistent support for recovery (not just acute diarrhea management):
- Saccharomyces boulardii CNCM I-745 — a non-pathogenic yeast that survives stomach acid, transiently colonizes the gut, displaces pathogens, and competes for adhesion sites. The Feizizadeh meta-analysis (PMID 24958586, 22 RCTs) showed roughly a 24-hour shortening of acute diarrhea; Dinleyici 2020 (PMID 32796401) extended this to post-acute recovery.
- Lactobacillus rhamnosus GG (LGG) — the most-studied probiotic strain in pediatric gastroenteritis. The Szajewska 2019 meta-analysis (PMID 31025399) showed a ~0.85-day shortening of diarrhea duration, though two large 2018 NEJM trials (Schnadower; Freedman) found no benefit in the emergency-department acute-care setting. The honest read: LGG appears useful for post-acute recovery support, less proven for stopping an acute attack.
For PI-IBS specifically, the Guandalini 2010 trial in children (PMID 20453678) showed that a high-dose multi-strain probiotic (the De Simone Formulation, sold as Visbiome) significantly improved pediatric IBS symptoms — abdominal pain, bloating, stool patterns — versus placebo.
Practical pick for an 11-year-old: Either a daily S. boulardii product (5-10 billion CFU) or a multi-strain pediatric probiotic with both Lactobacillus and Bifidobacterium species (10-25 billion CFU). Some clinicians stack S. boulardii morning + multi-strain evening for the first 4-6 weeks.
Pillar 2: L-Glutamine
The evidence: The Zhou 2019 RCT (PMID 30108163) is the strongest single-intervention trial in PI-IBS recovery. 5 grams three times daily (15 g/day) resolved diarrhea-predominant PI-IBS in 80% of adults at 8 weeks, versus 6% on placebo. Pediatric data are absent, but the safety profile of glutamine is excellent and the mechanism (enterocyte fuel, tight junction protein substrate) translates directly.
Practical pick for an 11-year-old: 2-3 g of L-glutamine powder, twice daily, dissolved in water or juice. Tasteless. Stop at 6-8 weeks; this is a recovery aid, not a permanent supplement.
Pillar 3: Partially Hydrolyzed Guar Gum (PHGG / Sunfiber)
The evidence: Niv 2016 (PMID 26855665), Yasukawa 2019 (PMID 31509971), and several smaller pediatric studies converge on the same finding: PHGG normalizes stool consistency in both directions, feeds Bacteroidetes, raises Bifidobacterium abundance, and improves IBS symptom scores.
Practical pick for an 11-year-old: 3-6 g/day of Sunfiber, mixed into morning yogurt, smoothie, or even soup. Tasteless. Continue for 8-12 weeks (or longer; PHGG is safe long-term).
Pillar 4: Mucosal Protectants and Gut-Barrier Support
This category covers the gentle demulcents and barrier-support supplements that round out the protocol:
- Slippery elm bark (Ulmus rubra) — mucilage polysaccharides form a colloidal coating over irritated mucosa. Traditional use, weak clinical evidence (Hawrelak pilot, 2010), excellent safety record. Lozenges or powder in warm water.
- Marshmallow root (Althaea officinalis) — same demulcent mechanism, longer pediatric herbal tradition, often gentler on the palate. Tea or cold-infusion overnight.
- Zinc carnosine (PepZinGI) — well-studied for adult gut barrier integrity (Mahmood 2007, PMID 16777920) but no pediatric RCTs. Use cautiously, lower doses for kids (~37.5 mg adult dose → ~15-20 mg for an 11-year-old, ideally with food).
- Bone broth — the evidence is mechanistic, not RCT-based. Glycine, glutamine, proline, gelatin. Treat it as a comforting food that happens to contain useful building blocks, not as a clinically proven therapy. But it is genuinely, deeply soothing, and an 11-year-old will often accept a bowl of chicken-broth-and-rice soup when nothing else sounds appealing.
Pillar 5: Dietary Reset
We covered the specifics above. The summary version:
- Add: cooked vegetables, lean protein, easy starches, olive oil, hard cheese, eggs, smoothies with PHGG.
- Pause (4-6 weeks, not forever): big dairy loads, onion/garlic, raw cruciferous, apple juice, beans, sugar alcohols.
- Consider a 2-week strict low-FODMAP trial at week 4-6 if the basic stack hasn't resolved things — followed by structured reintroduction.
Pillar 6: Vagal Tone and Cognitive Framing
This is the pillar most overlooked and arguably the most important for the anticipatory-anxiety pattern. Three practices:
- Name the loop. Explain it in kid-friendly language. The fluttery feeling is expected and meaningless — the body is over-anticipating because of a few weeks of bad experiences.
- Slow exhale breathing. Four-second inhale, six-to-eight-second exhale, for two minutes, before bathroom transitions or stressful eating moments. Lowers sympathetic tone fast.
- No avoidance. Gentle, gradual re-engagement with bathrooms outside the home. Praise for trying, no pressure, no negotiation. The loop dies when re-exposure outpaces avoidance.
For older kids who can engage with it, a structured app like Nerva (a Monash University-developed pediatric/adolescent gut-directed hypnotherapy program with RCT support in adult IBS) is worth considering at week 6-8 if symptoms persist.
Part XI: Homeopathic Adjuncts
Homeopathy has weak RCT evidence in pediatric PI-IBS specifically — most controlled trials in childhood diarrhea (Jacobs et al.) have studied acute, not post-infectious, settings. But the traditional materia medica offers a remarkably well-mapped set of indications, and many parents who lean toward integrative approaches will want this information available.
We present these as traditional usage — not as proven therapy — for families who want to use them alongside the evidence-backed stack.
| Remedy | Traditional indication | When to consider |
|---|---|---|
| Argentum nitricum | Anticipatory anxiety, hurriedness, diarrhea before stressful events, "fluttering" sensation | The closest single remedy to the gut-brain pattern described in this guide |
| Aloe (socotrina) | Sudden urgency, "insecurity of the rectum," gurgling, must run | The classic urgency-with-loose-stool remedy |
| Podophyllum | Profuse, gushing, painless morning diarrhea | Less specific but a long-time pediatric standby |
| Pulsatilla | Changeable stools — "no two alike" — worse after rich food, mild weepy temperament | Excellent constitutional match for many children |
| Gambogia | Sudden, violent, gushing diarrhea (less anxious component) | Acute rather than recovery use |
For families using homeopathic remedies, Boiron single remedies (30C is the most common pediatric potency) and Newton's Homeopathics combination formulas (their Bowel ~ Diarrhea combination contains several of the above) are the most widely available and well-quality-controlled.
Standard pediatric dosing: 3-5 pellets dissolved under the tongue, away from food and strong flavors (mint toothpaste, coffee), 2-3 times daily during active symptoms, tapering as improvement comes.
Part XII: Recommended Products
Starter Protocol for an 11-Year-Old with the Anticipatory-Anxiety Pattern
This is what the full six-pillar stack would look like over 8 weeks for the case at the top of this article. Dosing is conservative; adjust upward only if needed and tolerated.
Daily, all 8 weeks:
- Morning: S. boulardii (5 billion CFU) + 3 g PHGG mixed into yogurt or smoothie
- With lunch: 2 g L-glutamine powder in water
- Evening: Multi-strain probiotic (10 billion CFU, Lactobacillus + Bifidobacterium) + 2 g L-glutamine
Dietary, weeks 1-6:
- Lactose-free dairy (or hard-aged cheese / yogurt only)
- Pause onion, garlic, raw cruciferous, apple juice, beans, sugar alcohols
- Add: eggs, avocado, cooked vegetables, lean protein, sourdough/rice, olive oil, bone broth, berries
Twice daily (with active symptoms):
- 3-5 pellets Argentum nitricum 30C or Newton's Bowel ~ Diarrhea
Daily, all 8 weeks:
- 2-minute slow-exhale breathing practice (parent or child, ideally together)
- Reassurance: name the loop, no pressure, gradual re-exposure to outside bathrooms
Week 4 check-in: if Bristol score variance still high and bowel pattern still erratic, consider a 2-week low-FODMAP trial with structured reintroduction in weeks 6-8.
Stop point: most of the stack can be tapered off at week 8-10 once symptoms have been stable for 2-3 weeks. PHGG can continue indefinitely as it is essentially food.
Probiotics
- Florastor Kids — Saccharomyces boulardii CNCM I-745, the most-studied strain. 250 mg sachets, mix into food.
- Klaire Labs Ther-Biotic for Infants/Children — multi-strain, high-quality professional-grade, Lactobacillus + Bifidobacterium mix.
- Visbiome (formerly VSL#3) — the De Simone formulation studied in the Guandalini 2010 pediatric IBS RCT.
- Mercola Complete Probiotics Kids — clean, multi-strain pediatric option from a preferred brand.
Soluble Fiber + Gut Barrier Supports
- Tomorrow's Nutrition Sunfiber — pure PHGG, tasteless, the most-studied form.
- NOW Sunfiber — same ingredient, more economical.
- Pure Encapsulations L-Glutamine Powder — pharmaceutical-grade, no fillers.
- Jarrow PepZinGI (Zinc Carnosine) — the studied form.
- Mountain Rose Herbs Slippery Elm Bark — organic, bulk, can be made into a porridge.
- Mountain Rose Herbs Marshmallow Root — cold-infuse overnight for a gentle pediatric demulcent tea.
Homeopathic Remedies
- Boiron Argentum Nitricum 30C — single remedy, the closest match for anticipatory-anxiety patterns.
- Newton's Bowel ~ Diarrhea — combination formula covering several of the above traditional indications. Per family preference.
- Boiron Pulsatilla 30C — for the changeable-stool pattern.
Part XIII: When to See a Doctor
The vast majority of children with the picture described in this article — alternating soft and loose stools, no weight loss, no fever, no blood, no severe pain — have textbook post-infectious functional gut symptoms that will resolve, faster with support and eventually without. But there are red flags that warrant medical evaluation rather than home protocols.
See a pediatrician or pediatric gastroenterologist if any of these appear:
- Blood in the stool (bright red on the surface, dark/tarry, or mixed in)
- Fever above 100.4°F (38°C) lasting more than 24-48 hours after the acute illness ended
- Weight loss of more than 5% from pre-illness baseline, or any drop in growth percentile sustained over 6+ weeks
- Persistent abdominal pain (especially night pain, or pain that wakes the child from sleep)
- Persistent vomiting beyond the acute phase
- Symptoms that worsen rather than improve over weeks
- Symptoms that persist beyond 8-12 weeks with full support in place
- Signs of dehydration: reduced urine output, dry mouth, lethargy, dark circles
- New food intolerance that doesn't resolve in 6-8 weeks (concern for celiac, eosinophilic enteritis, or other secondary disease)
- Any sense from the parent that something is more wrong than this guide accounts for. Trust that instinct. A pediatric GI consult and stool studies (calprotectin, occult blood, ova and parasites, sometimes giardia antigen) can rule out the things this guide does not address.
Part XIV: The Honest Bottom Line
A child whose gut is taking a month or two to fully recover from a viral stomach bug is doing something that humans have been doing for at least 3,500 years. The biology is well-mapped. The natural history is reassuring. And the interventions that genuinely accelerate the recovery are cheap, safe, and broadly available.
The biggest single mistake families make is doing nothing for too long, then panicking at week 6 and starting four interventions at once. The next biggest mistake is doing nothing about the gut-brain loop — the anticipatory-anxiety component — which is the most fixable part of the whole picture and often the part that, left unaddressed, turns a 6-week problem into a 6-month one.
The second-biggest mistake is eliminating foods permanently that the child will tolerate again in 4-6 weeks (dairy especially, but also FODMAPs in general) — which carries a real nutritional and growth cost in exchange for a marginal recovery-time gain.
The third-biggest mistake is assuming probiotics and "gut health" supplements are interchangeable. They are not. Strain matters. The Florastor in the cabinet is not the same molecule as the multi-strain pediatric formula. The PHGG in your smoothie is not the same as the psyllium husk in your dad's morning routine. Match the molecule to the mechanism.
A child with the picture described at the top of this article — alternating loose and semi-formed stools, no weight loss, no fever, no blood, no severe pain, perhaps a quiet new anticipatory anxiety — has every biological reason to be fully recovered within 8-12 weeks. With the protocol laid out here, the recovery can be substantially faster, and the bathroom-anxiety loop can be unwound deliberately rather than allowed to entrench. That is, in practice, what a worried parent at week four actually needs to know.
References
The PMIDs throughout this article link to the primary peer-reviewed sources. Key references organized by topic:
Epidemiology and natural history of PI-IBS:
- Klem F, et al. "Prevalence, Risk Factors, and Outcomes of Irritable Bowel Syndrome After Infectious Enteritis: A Systematic Review and Meta-analysis." Gastroenterology 2017. PMID 28069350.
- Thabane M, Kottachchi DT, Marshall JK. "Systematic review and meta-analysis: The incidence and prognosis of post-infectious irritable bowel syndrome." Aliment Pharmacol Ther 2007. PMID 17661757.
- Spiller R, Garsed K. "Postinfectious irritable bowel syndrome." Gastroenterology 2009. PMID 19457422.
- Saps M, et al. "Post-infectious functional gastrointestinal disorders in children." J Pediatr 2008. PMID 20179687.
Probiotics (pediatric):
- Feizizadeh S, et al. "Efficacy and safety of Saccharomyces boulardii for acute diarrhea." Pediatrics 2014. PMID 24958586.
- Dinleyici EC, et al. "Saccharomyces boulardii CNCM I-745 in pediatric acute gastroenteritis." 2020. PMID 32796401.
- Szajewska H, et al. "Lactobacillus rhamnosus GG for the treatment of acute gastroenteritis in children: updated systematic review with meta-analysis." Aliment Pharmacol Ther 2019. PMID 31025399.
- Guandalini S, et al. "VSL#3 improves symptoms in children with irritable bowel syndrome: a multicenter, randomized, placebo-controlled, double-blind, crossover study." J Pediatr Gastroenterol Nutr 2010. PMID 20453678.
L-glutamine:
- Zhou Q, Verne ML, Fields JZ, et al. "Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome." Gut 2019. PMID 30108163.
Partially hydrolyzed guar gum (PHGG):
- Niv E, et al. "Randomized clinical study: Partially hydrolyzed guar gum (PHGG) versus placebo in the treatment of patients with irritable bowel syndrome." Nutr Metab 2016. PMID 26855665.
- Yasukawa Z, et al. "Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota." Nutrients 2019. PMID 31509971.
Zinc carnosine and gut barrier:
- Mahmood A, et al. "Zinc carnosine, a health food supplement that stabilises small bowel integrity." Gut 2007. PMID 16777920.
Lactose intolerance post-gastroenteritis:
- MacGillivray S, Fahey T, McGuire W. "Lactose avoidance for young children with acute diarrhoea." Cochrane Database 2013. PMID 25587230.
Low-FODMAP in pediatric IBS:
- Chumpitazi BP, Cope JL, Hollister EB, et al. "Randomised clinical trial: gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with irritable bowel syndrome." Aliment Pharmacol Ther 2015. PMID 26104013.
- Chumpitazi BP, et al. "Bristol Stool Form Scale and FODMAP responder identification in pediatric IBS." J Pediatr Gastroenterol Nutr 2018. PMID 28970147.
This article is a parent-and-clinician-facing educational guide. It is not a substitute for individual medical advice. The protocols described should be discussed with your child's pediatrician or pediatric gastroenterologist, particularly if any of the red-flag symptoms listed in Part XIII apply.